

Gender as a Modifying Factor Influencing Myotonic Dystrophy Type 1 Phenotype Severity and Mortality: A Nationwide Multiple Databases Cross-Sectional Observational Study
- PMID: 26849574
- PMCID: PMC4744025
- DOI: 10.1371/journal.pone.0148264
Gender as a Modifying Factor Influencing Myotonic Dystrophy Type 1 Phenotype Severity and Mortality: A Nationwide Multiple Databases Cross-Sectional Observational Study
Abstract
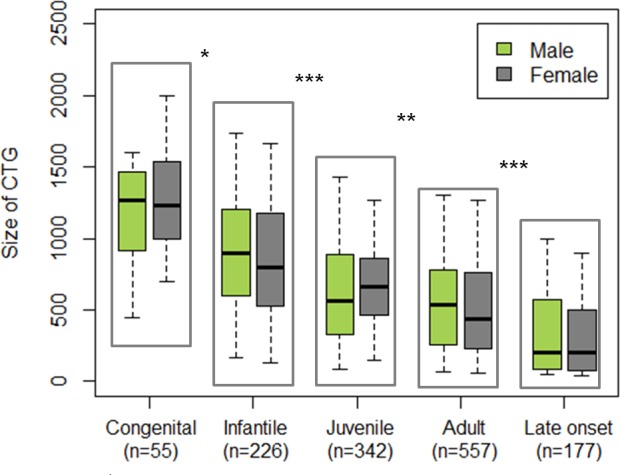
Background: Myotonic Dystrophy type 1 (DM1) is one of the most heterogeneous hereditary disease in terms of age of onset, clinical manifestations, and severity, challenging both medical management and clinical trials. The CTG expansion size is the main factor determining the age of onset although no factor can finely predict phenotype and prognosis. Differences between males and females have not been specifically reported. Our aim is to study gender impact on DM1 phenotype and severity.
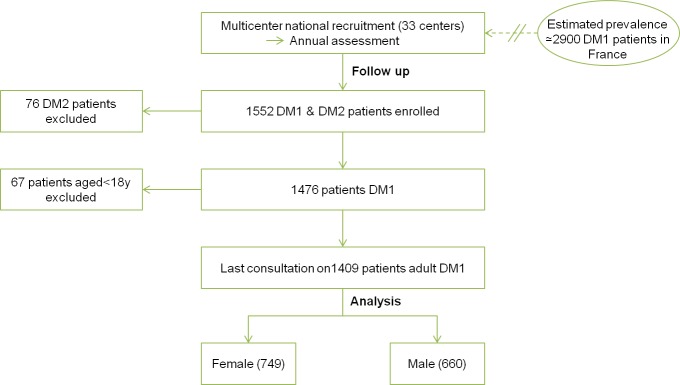
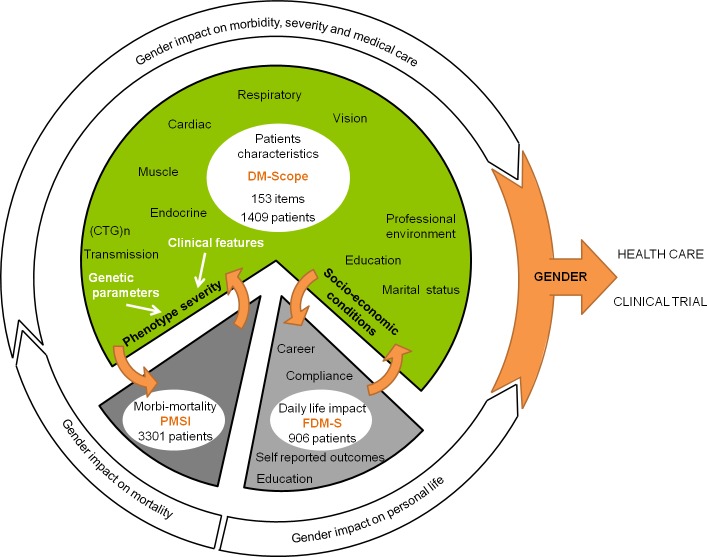
Methods: We first performed cross-sectional analysis of main multiorgan clinical parameters in 1409 adult DM1 patients (>18 y) from the DM-Scope nationwide registry and observed different patterns in males and females. Then, we assessed gender impact on social and economic domains using the AFM-Téléthon DM1 survey (n = 970), and morbidity and mortality using the French National Health Service Database (n = 3301).
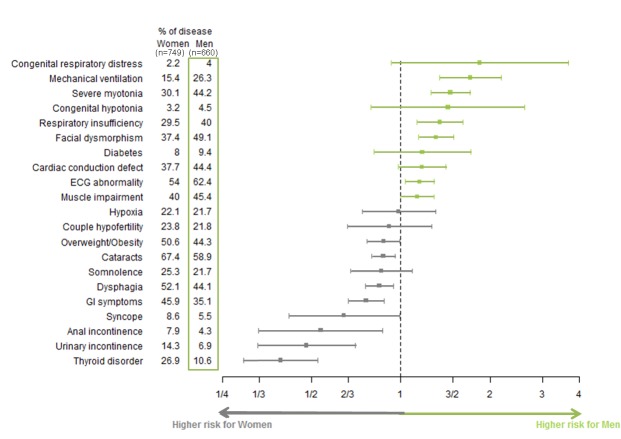
Results: Men more frequently had (1) severe muscular disability with marked myotonia, muscle weakness, cardiac, and respiratory involvement; (2) developmental abnormalities with facial dysmorphism and cognitive impairment inferred from low educational levels and work in specialized environments; and (3) lonely life. Alternatively, women more frequently had cataracts, dysphagia, digestive tract dysfunction, incontinence, thyroid disorder and obesity. Most differences were out of proportion to those observed in the general population. Compared to women, males were more affected in their social and economic life. In addition, they were more frequently hospitalized for cardiac problems, and had a higher mortality rate.
Conclusion: Gender is a previously unrecognized factor influencing DM1 clinical profile and severity of the disease, with worse socio-economic consequences of the disease and higher morbidity and mortality in males. Gender should be considered in the design of both stratified medical management and clinical trials.
Conflict of interest statement
Figures
References
-
- Pinessi L, Bergamini L, Cantello R, Di Tizio C. Myotonia congenita and myotonic dystrophy: descriptive epidemiological investigation in Turin. Ital J Neurol Sci. 1982. October;3(3):207–10. - PubMed
-
- Mathieu J, De Braekeleer M, Prevost C. Genealogical reconstruction of myotonic dystrophy in the Saguenay-Lac-Saint-Jean area (Quebec, Canada). Neurology. 1990. May;40(5):839–42. - PubMed
-
- Harper P. Myotonic Dystrophy, 3rd Edition-Major Problems in Neurology. In: Medicine; 2001.
-
- Aslanidis C, Jansen G, Amemiya C, Shutler G, Mahadevan M, Tsilfidis C et al. Cloning of the essential myotonic dystrophy region and mapping of the putative defect. Nature. 1992. February 6;355(6360):548–51. - PubMed
-
- Brook JD, McCurrach ME, Harley HG, Buckler AJ, Church D, Aburatani H et al. Molecular basis of myotonic dystrophy: expansion of a trinucleotide (CTG) repeat at the 3' end of a transcript encoding a protein kinase family member. Cell. 1992. February 21;68(4):799–808. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
