

Integrated systems of stroke care and reduction in 30-day mortality: A retrospective analysis
- PMID: 26850979
- PMCID: PMC4782112
- DOI: 10.1212/WNL.0000000000002443
Integrated systems of stroke care and reduction in 30-day mortality: A retrospective analysis
Abstract
Objective: To evaluate the association between the presence of integrated systems of stroke care and stroke case-fatality across Canada.
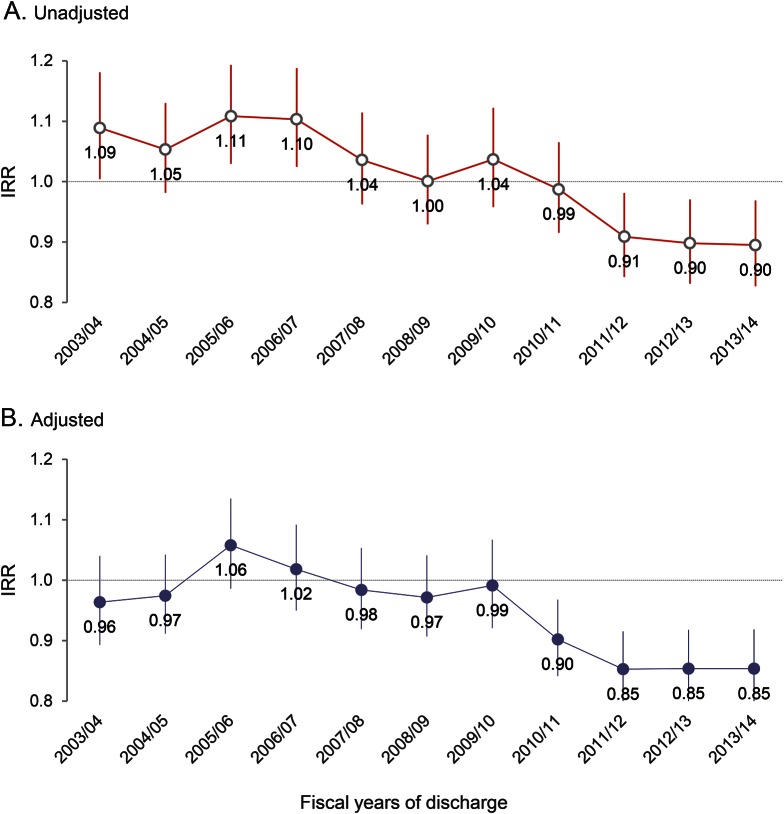
Methods: We used the Canadian Institute of Health Information's Discharge Abstract Database to retrospectively identify a cohort of stroke/TIA patients admitted to all acute care hospitals, excluding the province of Quebec, in 11 fiscal years from 2003/2004 to 2013/2014. We used a modified Poisson regression model to compute the adjusted incidence rate ratio (aIRR) of 30-day in-hospital mortality across time for provinces with stroke systems compared to those without, controlling for age, sex, stroke type, comorbidities, and discharge year. We conducted surveys of stroke care resources in Canadian hospitals in 2009 and 2013, and compared resources in provinces with integrated systems to those without.
Results: A total of 319,972 patients were hospitalized for stroke/TIA. The crude 30-day mortality rate decreased from 15.8% in 2003/2004 to 12.7% in 2012/2013 in provinces with stroke systems, while remaining 14.5% in provinces without such systems. Starting with the fiscal year 2009/2010, there was a clear reduction in relative mortality in provinces with stroke systems vs those without, sustained at aIRR of 0.85 (95% confidence interval 0.79-0.92) in the 2011/2012, 2012/2013, and 2013/2014 fiscal years. The surveys indicated that facilities in provinces with such systems were more likely to care for patients on a stroke unit, and have timely access to a stroke prevention clinic and telestroke services.
Conclusion: In this retrospective study, the implementation of integrated systems of stroke care was associated with a population-wide reduction in mortality after stroke.
© 2016 American Academy of Neurology.
Figures
Comment in
-
Stroke systems of care: The sum is greater than the parts.Neurology. 2016 Mar 8;86(10):886-7. doi: 10.1212/WNL.0000000000002452. Epub 2016 Feb 5. Neurology. 2016. PMID: 26850980 No abstract available.
References
-
- Alberts M, Latchaw R, Selman W, et al. Recommendations for comprehensive stroke centers: a consensus statement from the Brain Attack Coalition. Stroke 2005;36:1597–1616. - PubMed
-
- Schwamm L, Pancioli A, Acker JR, et al. Recommendations for the establishment of stroke systems of care: recommendations from the American Stroke Association's Task Force on the Development of Stroke Systems. Stroke 2005;36:690–703. - PubMed
-
- Lewis S. A system in name only: access, variation, and reform in Canada's provinces. N Engl Journal Med 2015;372:497–500. - PubMed
-
- Mamdani M, Tu J. Appendix 5: Emergency/Acute Stroke Task Group Economic Decision Analysis Model. Toronto: Ontario Ministry of Health and Long-Term Care; 2000.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical