

Estimating the Severity and Subclinical Burden of Middle East Respiratory Syndrome Coronavirus Infection in the Kingdom of Saudi Arabia
- PMID: 26851269
- PMCID: PMC4801139
- DOI: 10.1093/aje/kwv452
Estimating the Severity and Subclinical Burden of Middle East Respiratory Syndrome Coronavirus Infection in the Kingdom of Saudi Arabia
Abstract
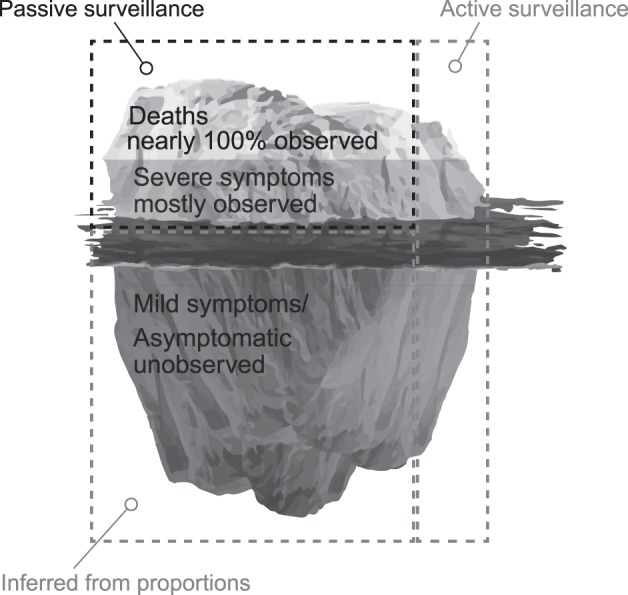
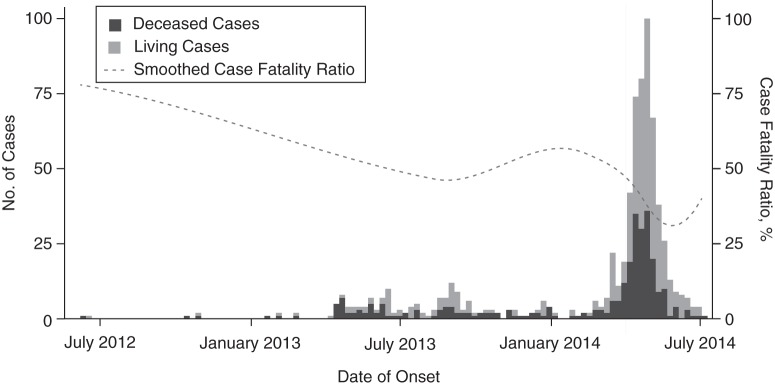
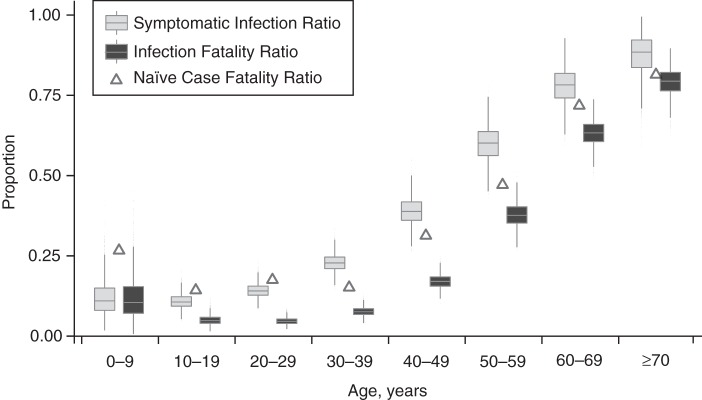
Not all persons infected with Middle East respiratory syndrome coronavirus (MERS-CoV) develop severe symptoms, which likely leads to an underestimation of the number of people infected and an overestimation of the severity. To estimate the number of MERS-CoV infections that have occurred in the Kingdom of Saudi Arabia, we applied a statistical model to a line list describing 721 MERS-CoV infections detected between June 7, 2012, and July 25, 2014. We estimated that 1,528 (95% confidence interval (CI): 1,327, 1,883) MERS-CoV infections occurred in this interval, which is 2.1 (95% CI: 1.8, 2.6) times the number reported. The probability of developing symptoms ranged from 11% (95% CI: 4, 25) in persons under 10 years of age to 88% (95% CI: 72, 97) in those 70 years of age or older. An estimated 22% (95% CI: 18, 25) of those infected with MERS-CoV died. MERS-CoV is deadly, but this work shows that its clinical severity differs markedly between groups and that many cases likely go undiagnosed.
Keywords: MERS; burden; clinical symptoms; coronavirus; severity.
© The Author 2016. Published by Oxford University Press on behalf of the Johns Hopkins Bloomberg School of Public Health. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Figures
References
-
- Gulland A. WHO voices concern over rising numbers of MERS-CoV cases. BMJ. 2014;348:g2968. - PubMed
-
- World Health Organization. Middle East Respiratory Syndrome Coronavirus (MERS-CoV) Summary and Literature Update—as of 9 May 2014. Geneva, Switzerland: World Health Organization; 2014.
-
- World Health Organization. Middle East respiratory syndrome coronavirus (MERS-CoV). Fact sheet No. 401. June 2015 http://www.who.int/mediacentre/factsheets/mers-cov/en/ Accessed December 16, 2015.
-
- Shrestha SS, Swerdlow DL, Borse RH et al. . Estimating the burden of 2009 pandemic influenza A (H1N1) in the United States (April 2009–April 2010). Clin Infect Dis. 2011;52(suppl 1):S75–S82. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
