

Removing and reimplanting deep brain stimulation therapy devices in resistant OCD (when the patient does not respond): case report
- PMID: 26852116
- PMCID: PMC4744631
- DOI: 10.1186/s12888-016-0730-z
Removing and reimplanting deep brain stimulation therapy devices in resistant OCD (when the patient does not respond): case report
Abstract
Background: Deep brain stimulation (DBS) is emerging as a promising tool in the treatment of refractory obsessive-compulsive disorder (OCD) but the search for the best target still continues. This issue is especially relevant when particularly resistant profiles are observed in some patients, which have been ascribed to individual responses to DBS according to differential patterns of connectivity. As patients have been implanted, new dilemmas have emerged, such as what to do when the patient does not respond to surgery.
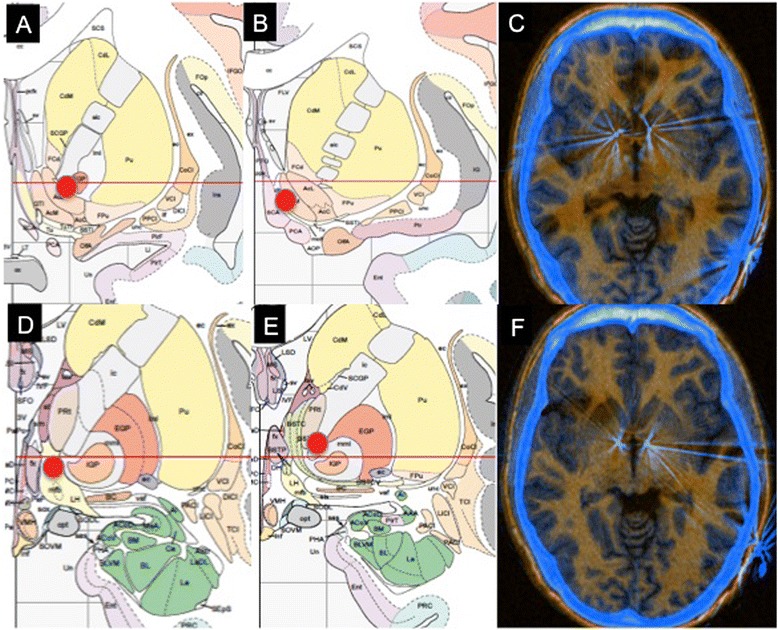
Case presentation: Here we describe a 22-year-old male with extremely severe OCD who did not respond to treatment with DBS in the nucleus accumbens, but who did respond after explanting and reimplanting leads targeting the ventral capsule-ventral striatum region. Information regarding the position of the electrodes for both surgeries is provided and possible brain structures affected during stimulation are reviewed. To our knowledge this case is the first in the literature reporting the removal and reimplantation of DBS leads for therapeutical benefits in a patient affected by a mental disorder.
Conclusion: The capability for explantation and reimplantation of leads should be considered as part of the DBS therapy reversibility profile in resistant mental disorders, as it allows application in cases of non-response to the first surgery.
Figures
Similar articles
-
Deep brain stimulation in the treatment of obsessive-compulsive disorder.World Neurosurg. 2013 Dec;80(6):e245-53. doi: 10.1016/j.wneu.2012.10.006. Epub 2012 Oct 5. World Neurosurg. 2013. PMID: 23044000 Review.
-
Combined bilateral anterior cingulotomy and ventral capsule/ventral striatum deep brain stimulation for refractory obsessive-compulsive disorder with major depression: do combined procedures have a long-term benefit?Restor Neurol Neurosci. 2013;31(6):723-32. doi: 10.3233/RNN-120290. Restor Neurol Neurosci. 2013. PMID: 23979095
-
Deep brain stimulation versus anterior capsulotomy for obsessive-compulsive disorder: a review of the literature.J Neurosurg. 2015 May;122(5):1028-37. doi: 10.3171/2014.11.JNS132618. Epub 2015 Jan 30. J Neurosurg. 2015. PMID: 25635480 Review.
-
Deep brain stimulation of the nucleus accumbens and bed nucleus of stria terminalis for obsessive-compulsive disorder: a case series.World Neurosurg. 2015 Apr;83(4):657-63. doi: 10.1016/j.wneu.2014.12.024. Epub 2014 Dec 18. World Neurosurg. 2015. PMID: 25527882
-
Anatomic Review of the Ventral Capsule/Ventral Striatum and the Nucleus Accumbens to Guide Target Selection for Deep Brain Stimulation for Obsessive-Compulsive Disorder.World Neurosurg. 2019 Jun;126:1-10. doi: 10.1016/j.wneu.2019.01.254. Epub 2019 Feb 18. World Neurosurg. 2019. PMID: 30790738 Review.
Cited by
-
Deep brain stimulation for obsessive compulsive disorder: A review of results by anatomical target.Ment Illn. 2018 Nov 6;10(2):7900. doi: 10.4081/mi.2018.7900. eCollection 2018 Nov 6. Ment Illn. 2018. PMID: 30542526 Free PMC article.
-
Ablative neurosurgery and deep brain stimulation for obsessive-compulsive disorder.Indian J Psychiatry. 2019 Jan;61(Suppl 1):S77-S84. doi: 10.4103/psychiatry.IndianJPsychiatry_523_18. Indian J Psychiatry. 2019. PMID: 30745680 Free PMC article. Review.
-
Deep Brain Stimulation for Refractory Obsessive-Compulsive Disorder: Towards an Individualized Approach.Front Psychiatry. 2019 Dec 13;10:905. doi: 10.3389/fpsyt.2019.00905. eCollection 2019. Front Psychiatry. 2019. PMID: 31920754 Free PMC article. Review.
-
Neurosurgery for mental conditions and pain: An historical perspective on the limits of biological determinism.Surg Neurol Int. 2024 Dec 27;15:479. doi: 10.25259/SNI_819_2024. eCollection 2024. Surg Neurol Int. 2024. PMID: 39777168 Free PMC article. Review.
References
-
- Greenberg BD, Rezai AR. Mechanisms and the current state of deep brain stimulation in neuropsychiatry. CNS Spectr. 2003;8:522–6. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
