

What is the value of reactive case detection in malaria control? A case-study in India and a systematic review
- PMID: 26852118
- PMCID: PMC4744450
- DOI: 10.1186/s12936-016-1120-1
What is the value of reactive case detection in malaria control? A case-study in India and a systematic review
Abstract
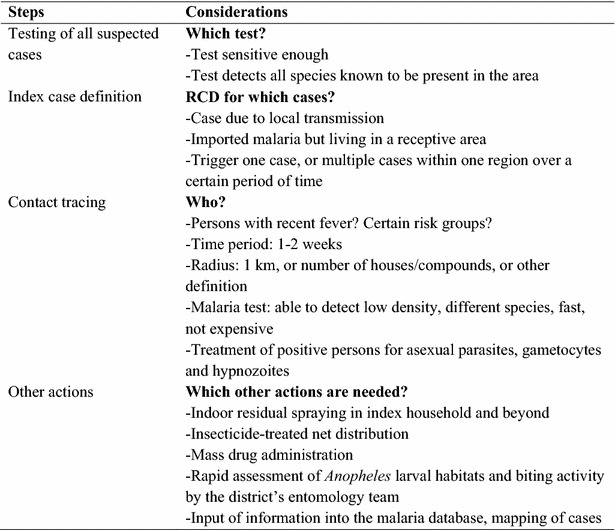
Background: Reactive case detection (RCD) for malaria is a strategy to identify additional malaria infections in areas of low malaria transmission and can complement passive surveillance. This study describes experiences with RCD in two Indian sites, and aimed to synthesize experiences with RCD across endemic countries.
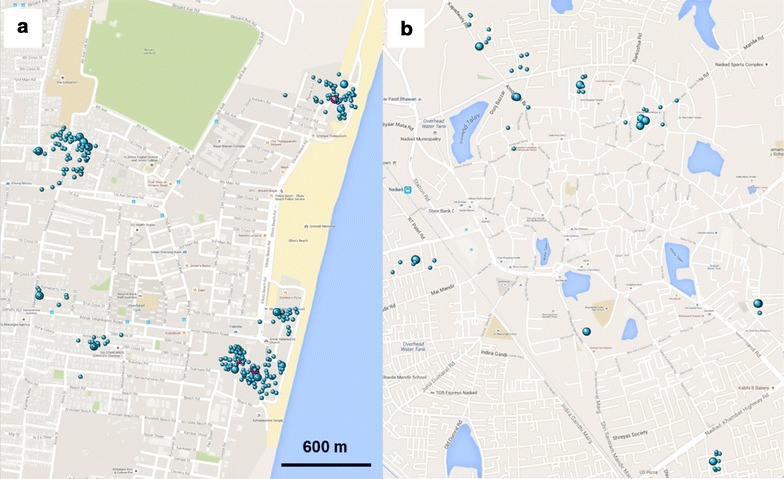
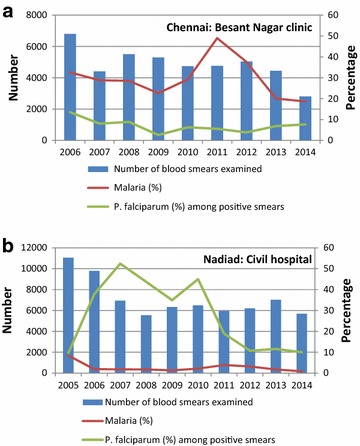
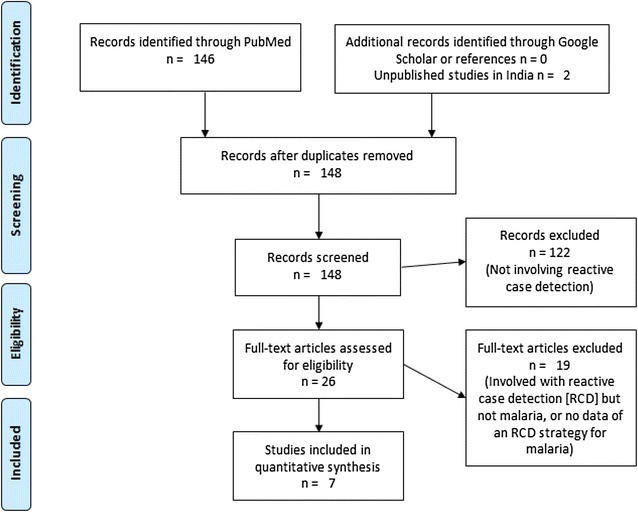
Methods: RCD programmes were piloted in two urban areas of India with a low prevalence of mainly Plasmodium vivax malaria in 2014. Cases were identified in a clinic by microscopy and contacts were screened within 2 weeks; PCR, in addition to microscopy, was used to detect Plasmodium parasites. A systematic review was conducted to identify RCD experiences in the literature.
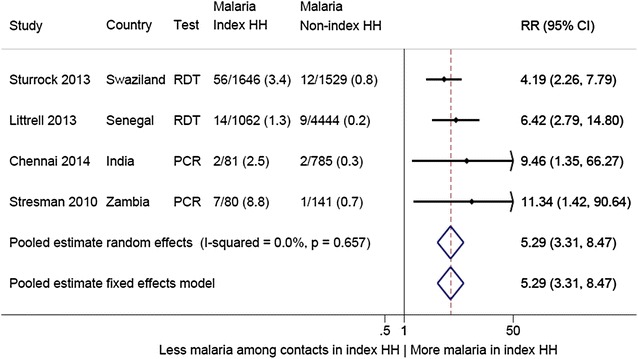
Results: In Chennai, 868 contacts were enrolled for 18 index cases of clinical malaria; in Nadiad, 131 contacts were enrolled for 20 index cases. No new malaria infections were detected in Nadiad among contacts, and four new infections were detected in Chennai (three P. vivax and one Plasmodium falciparum), of which two were among household members of index cases. An additional five studies describing results from an RCD strategy were identified in the literature: four in Africa and one in Thailand. Including the results from India, the average number of contacts screened per index case in a total of seven studies ranged from four to 50, and 126 in a case study in Thailand with one index case. Malaria was detected in 0-45 % of the contacted persons. The average number of index cases needed to be traced to find one new case of malaria ranged from one to five, and could not be assessed in one study in India (no contacts positive for 20 cases). Sharing the household with an index case was associated with a five-fold increased risk of malaria compared to contacts from households without an index case (pooled risk ratio 5.29, 95 % CI 3.31-8.47, I(2) 0 %, four studies).
Conclusions: RCD in areas of low malaria transmission is a labour-intensive strategy, and its benefit is not clear. Studies are needed to assess how RCD can be optimized or into alternatives where interventions are targeted to family members or hotspots.
Figures
Similar articles
-
Severe thrombocytopaenia in patients with vivax malaria compared to falciparum malaria: a systematic review and meta-analysis.Infect Dis Poverty. 2018 Feb 9;7(1):10. doi: 10.1186/s40249-018-0392-9. Infect Dis Poverty. 2018. PMID: 29427995 Free PMC article.
-
Indoor residual spraying for preventing malaria.Cochrane Database Syst Rev. 2010 Apr 14;2010(4):CD006657. doi: 10.1002/14651858.CD006657.pub2. Cochrane Database Syst Rev. 2010. PMID: 20393950 Free PMC article.
-
Mass drug administration for malaria.Cochrane Database Syst Rev. 2021 Sep 29;9(9):CD008846. doi: 10.1002/14651858.CD008846.pub3. Cochrane Database Syst Rev. 2021. PMID: 34585740 Free PMC article.
-
Primaquine for reducing Plasmodium falciparum transmission.Cochrane Database Syst Rev. 2012 Sep 12;(9):CD008152. doi: 10.1002/14651858.CD008152.pub2. Cochrane Database Syst Rev. 2012. Update in: Cochrane Database Syst Rev. 2014 Jun 30;(6):CD008152. doi: 10.1002/14651858.CD008152.pub3. PMID: 22972117 Updated.
-
Signs and symptoms to determine if a patient presenting in primary care or hospital outpatient settings has COVID-19.Cochrane Database Syst Rev. 2022 May 20;5(5):CD013665. doi: 10.1002/14651858.CD013665.pub3. Cochrane Database Syst Rev. 2022. PMID: 35593186 Free PMC article.
Cited by
-
Reactive Case Detection Strategy for Malaria Control and Elimination: A 12 Year Systematic Review and Meta-Analysis from 25 Malaria-Endemic Countries.Trop Med Infect Dis. 2023 Mar 18;8(3):180. doi: 10.3390/tropicalmed8030180. Trop Med Infect Dis. 2023. PMID: 36977181 Free PMC article. Review.
-
The impact of reactive case detection on malaria transmission in Zanzibar in the presence of human mobility.Epidemics. 2022 Dec;41:100639. doi: 10.1016/j.epidem.2022.100639. Epub 2022 Oct 20. Epidemics. 2022. PMID: 36343496 Free PMC article.
-
The Utility of Malaria Rapid Diagnostic Tests as a Tool in Enhanced Surveillance for Malaria Elimination in Vanuatu.PLoS One. 2016 Nov 30;11(11):e0167136. doi: 10.1371/journal.pone.0167136. eCollection 2016. PLoS One. 2016. PMID: 27902755 Free PMC article.
-
Reactive Case Detection and Treatment and Reactive Drug Administration for Reducing Malaria Transmission: A Systematic Review and Meta-Analysis.Am J Trop Med Hyg. 2023 Dec 20;110(4_Suppl):82-93. doi: 10.4269/ajtmh.22-0720. Print 2024 Apr 2. Am J Trop Med Hyg. 2023. PMID: 38118166 Free PMC article.
-
Malaria risk factor assessment using active and passive surveillance data from Aceh Besar, Indonesia, a low endemic, malaria elimination setting with Plasmodium knowlesi, Plasmodium vivax, and Plasmodium falciparum.Malar J. 2016 Sep 13;15(1):468. doi: 10.1186/s12936-016-1523-z. Malar J. 2016. PMID: 27619000 Free PMC article.
References
-
- WHO. Achieving the malaria MDG Target: reversing the incidence of malaria 2000–2015. Geneva, Switzerland: World Health Organization; 2015.
-
- Ohrt C, Roberts K, Sturrock HJ, Wegbreit J, Gosling R, Lee B. Surveillance systems to facilitate malaria elimination. San Francisco: UCSF Global Health Sciences Global Health Group; 2014.
-
- WHO. Disease surveillance for malaria elimination: an operational manual. Geneva, Switzerland: World Health Organization; 2012.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
