

Intestinal Microbiota Distinguish Gout Patients from Healthy Humans
- PMID: 26852926
- PMCID: PMC4757479
- DOI: 10.1038/srep20602
Intestinal Microbiota Distinguish Gout Patients from Healthy Humans
Abstract
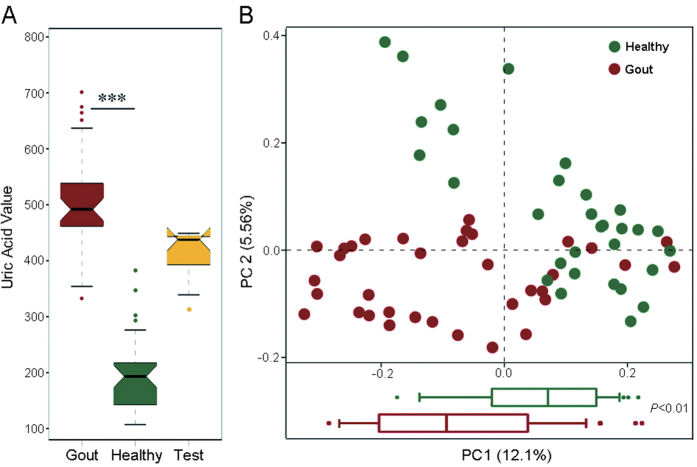
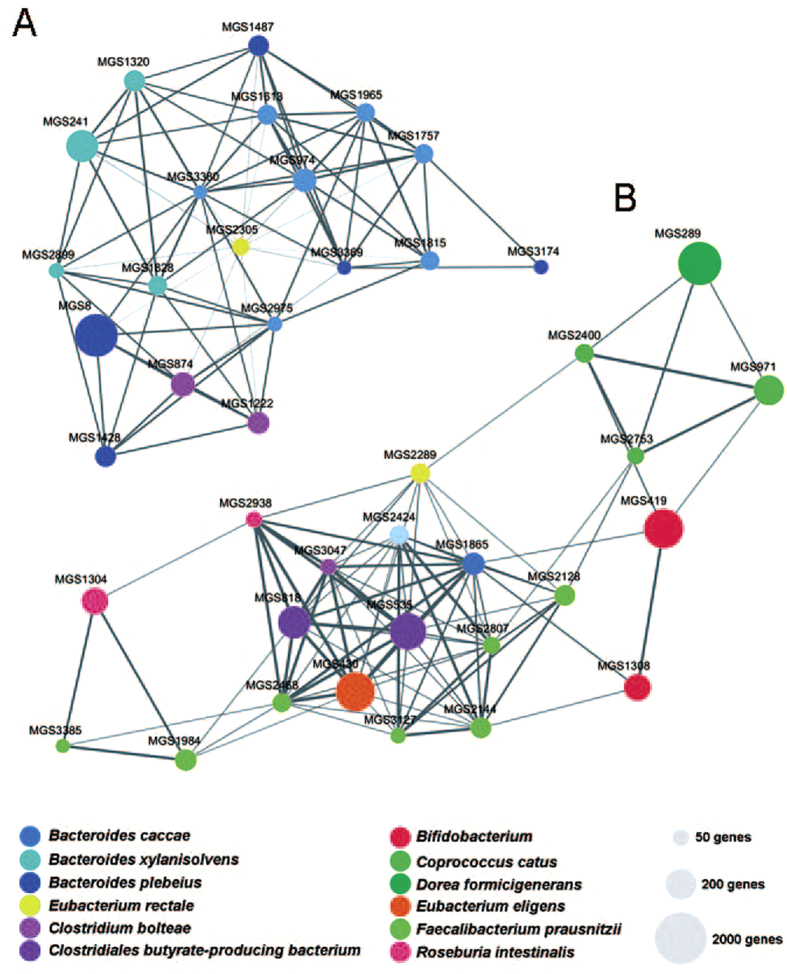
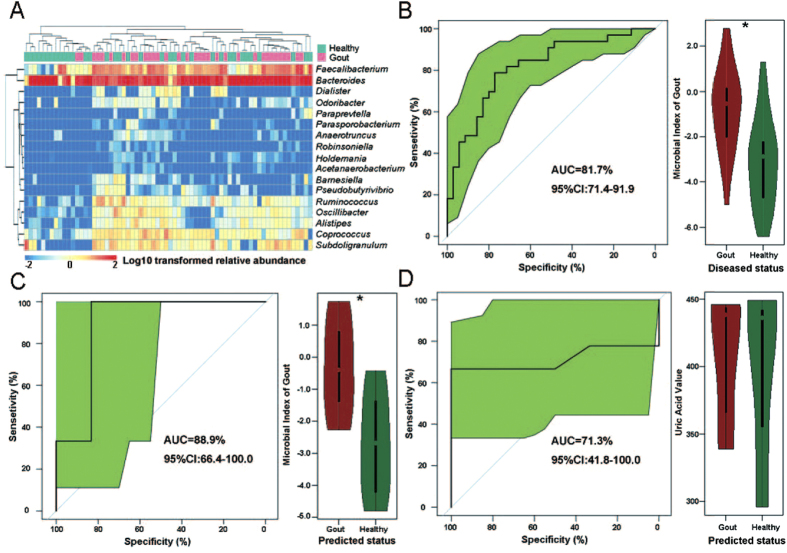
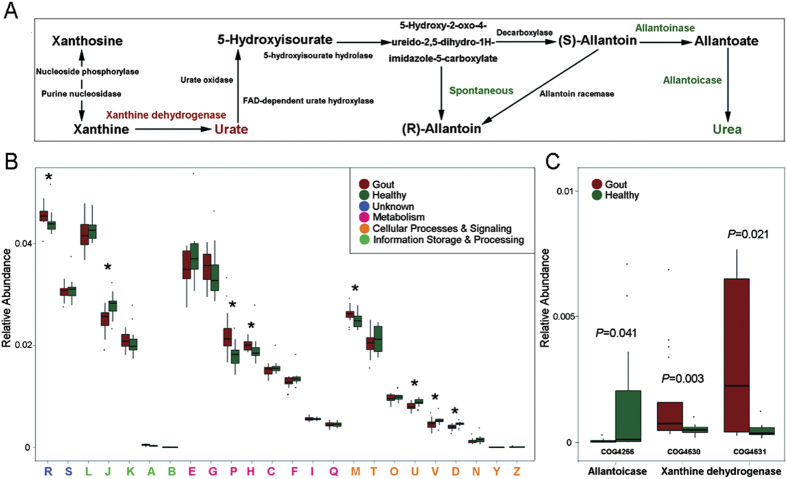
Current blood-based approach for gout diagnosis can be of low sensitivity and hysteretic. Here via a 68-member cohort of 33 healthy and 35 diseased individuals, we reported that the intestinal microbiota of gout patients are highly distinct from healthy individuals in both organismal and functional structures. In gout, Bacteroides caccae and Bacteroides xylanisolvens are enriched yet Faecalibacterium prausnitzii and Bifidobacterium pseudocatenulatum depleted. The established reference microbial gene catalogue for gout revealed disorder in purine degradation and butyric acid biosynthesis in gout patients. In an additional 15-member validation-group, a diagnosis model via 17 gout-associated bacteria reached 88.9% accuracy, higher than the blood-uric-acid based approach. Intestinal microbiota of gout are more similar to those of type-2 diabetes than to liver cirrhosis, whereas depletion of Faecalibacterium prausnitzii and reduced butyrate biosynthesis are shared in each of the metabolic syndromes. Thus the Microbial Index of Gout was proposed as a novel, sensitive and non-invasive strategy for diagnosing gout via fecal microbiota.
Figures
References
-
- Burns C. M. & Wortmann R. L. Gout therapeutics: new drugs for an old disease. Lancet 377, 165–177 (2011). - PubMed
-
- Richette P. & Bardin T. Gout. Lancet 375, 318–328 (2010). - PubMed
-
- Zhu Y., Pandya B. J. & Choi H. K. Comorbidities of gout and hyperuricemia in the US general population: NHANES 2007–2008. Am J Med 125, 679–687 (2012). - PubMed
-
- Guo M. et al. Polymorphism of rs7688672 and rs10033237 in cGKII/PRKG2 and gout susceptibility of Han population in northern China. Gene 562, 50–54 (2015). - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
