

Imaging of HCC-Current State of the Art
- PMID: 26854169
- PMCID: PMC4728473
- DOI: 10.3390/diagnostics5040513
Imaging of HCC-Current State of the Art
Abstract
Early diagnosis of hepatocellular carcinoma (HCC) is crucial for optimizing treatment outcome. Ongoing advances are being made in imaging of HCC regarding detection, grading, staging, and also treatment monitoring. This review gives an overview of the current international guidelines for diagnosing HCC and their discrepancies as well as critically summarizes the role of magnetic resonance imaging (MRI) and computed tomography (CT) techniques for imaging in HCC. The diagnostic performance of MRI with nonspecific and hepatobililiary contrast agents and the role of functional imaging with diffusion-weighted imaging will be discussed. On the other hand, CT as a fast, cheap and easily accessible imaging modality plays a major role in the clinical routine work-up of HCC. Technical advances in CT, such as dual energy CT and volume perfusion CT, are currently being explored for improving detection, characterization and staging of HCC with promising results. Cone beam CT can provide a three-dimensional analysis of the liver with tumor and vessel characterization comparable to cross-sectional imaging so that this technique is gaining an increasing role in the peri-procedural imaging of HCC treated with interventional techniques.
Keywords: computed tomography; contrast media; diffusion-weighted imaging; dual-energy computed tomography; dynamic contrast-enhanced magnetic resonance imaging; guidelines; hepatocellular carcinoma; hepatocyte specific contrast media; magnetic resonance imaging; volume perfusion computed tomography.
Figures
References
-
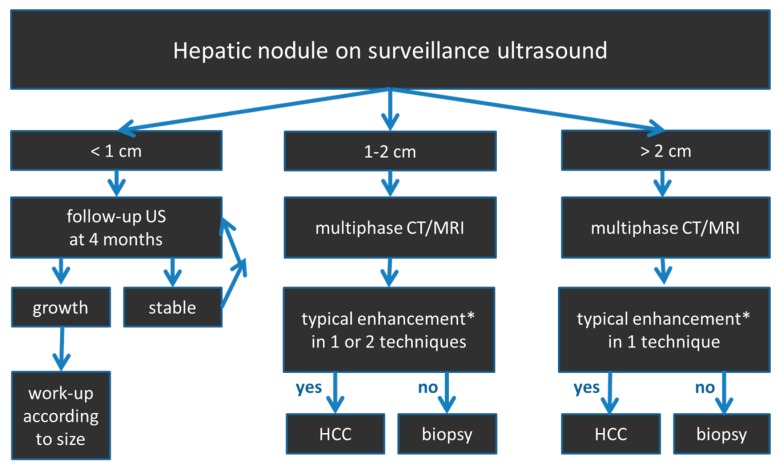
- European Association for the Study of the Liver EASL-EORTC clinical practice guidelines: Management of hepatocellular carcinoma. J. Hepatol. 2012;56:908–943. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
