

Diffuse Large B-Cell Lymphoma: Prospective Multicenter Comparison of Early Interim FLT PET/CT versus FDG PET/CT with IHP, EORTC, Deauville, and PERCIST Criteria for Early Therapeutic Monitoring
- PMID: 26854705
- PMCID: PMC4934532
- DOI: 10.1148/radiol.2015150689
Diffuse Large B-Cell Lymphoma: Prospective Multicenter Comparison of Early Interim FLT PET/CT versus FDG PET/CT with IHP, EORTC, Deauville, and PERCIST Criteria for Early Therapeutic Monitoring
Abstract
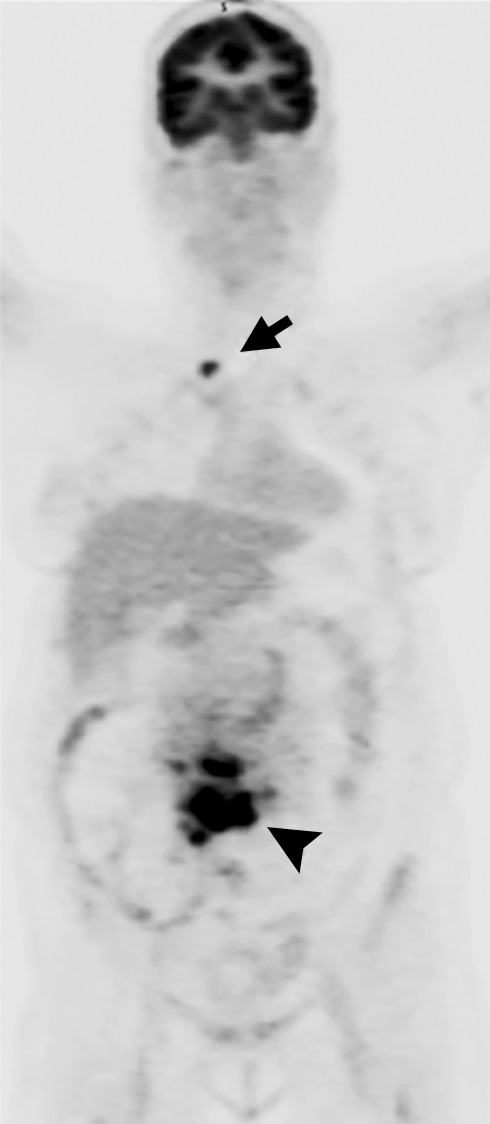
Purpose To compare the performance characteristics of interim fluorine 18 ((18)F) fluorodeoxyglucose (FDG) positron emission tomography (PET)/computed tomography (CT) (after two cycles of chemotherapy) by using the most prominent standardized interpretive criteria (including International Harmonization Project [IHP] criteria, European Organization for Research and Treatment of Cancer [EORTC] criteria, and PET Response Criteria in Solid Tumors (PERCIST) versus those of interim (18)F fluorothymidine (FLT) PET/CT and simple visual interpretation. Materials and Methods This HIPAA-compliant prospective study was approved by the institutional review boards, and written informed consent was obtained. Patients with newly diagnosed diffuse large B-cell lymphoma (DLBCL) underwent both FLT and FDG PET/CT 18-24 days after two cycles of rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone or rituximab, etoposide, prednisone, vincristine, cyclophosphamide, and doxorubicin. For FDG PET/CT interpretation, IHP criteria, EORTC criteria, PERCIST, Deauville criteria, standardized uptake value, total lesion glycolysis, and metabolic tumor volume were used. FLT PET/CT images were interpreted with visual assessment by two reviewers in consensus. The interim (after cycle 2) FDG and FLT PET/CT studies were then compared with the end-of-treatment FDG PET/CT studies to determine which interim examination and/or criteria best predicted the result after six cycles of chemotherapy. Results From November 2011 to May 2014, there were 60 potential patients for inclusion, of whom 46 patients (24 men [mean age, 60.9 years ± 13.7; range, 28-78 years] and 22 women [mean age, 57.2 years ± 13.4; range, 25-76 years]) fulfilled the criteria. Thirty-four patients had complete response, and 12 had residual disease at the end of treatment. FLT PET/CT had a significantly higher positive predictive value (PPV) (91%) in predicting residual disease than did any FDG PET/CT interpretation method (42%-46%). No difference in negative predictive value (NPV) was found between FLT PET/CT (94%) and FDG PET/CT (82%-95%), regardless of the interpretive criteria used. FLT PET/CT showed statistically higher (P < .001-.008) or similar NPVs than did FDG PET/CT. Conclusion Early interim FLT PET/CT had a significantly higher PPV than standardized FDG PET/CT-based interpretation for therapeutic response assessment in DLBCL. (©) RSNA, 2016 Online supplemental material is available for this article.
Figures







Similar articles
-
18F-Fluorothymidine PET is an early and superior predictor of progression-free survival following chemoimmunotherapy of diffuse large B cell lymphoma: a multicenter study.Eur J Nucl Med Mol Imaging. 2021 Aug;48(9):2883-2893. doi: 10.1007/s00259-021-05353-9. Epub 2021 Apr 28. Eur J Nucl Med Mol Imaging. 2021. PMID: 33909086 Free PMC article.
-
Prognostic value of interim FDG PET-CT in patients older than 60 years with diffuse large B-cell lymphoma treated by PMitCEBO plus rituximab. Comparison between Deauville 5-point scale and International Harmonization Project criteria.Q J Nucl Med Mol Imaging. 2021 Dec;65(4):402-409. doi: 10.23736/S1824-4785.16.02894-6. Epub 2016 Nov 30. Q J Nucl Med Mol Imaging. 2021. PMID: 35133099
-
Final Results of a Prospective Evaluation of the Predictive Value of Interim Positron Emission Tomography in Patients With Diffuse Large B-Cell Lymphoma Treated With R-CHOP-14 (SAKK 38/07).J Clin Oncol. 2015 Aug 10;33(23):2523-9. doi: 10.1200/JCO.2014.58.9846. Epub 2015 Jul 6. J Clin Oncol. 2015. PMID: 26150440
-
Bilateral primary renal lymphoma in a pediatric patient: staging and response evaluation with ¹⁸F-FDG PET/CT.Rev Esp Med Nucl Imagen Mol. 2015 Jan-Feb;34(1):49-52. doi: 10.1016/j.remn.2014.05.004. Epub 2014 Jul 21. Rev Esp Med Nucl Imagen Mol. 2015. PMID: 25065972 Review.
-
FDG-PET for Early Response Assessment in Lymphomas: Part 1-Hodgkin Lymphoma.Oncology (Williston Park). 2017 Jan 15;31(1):45-9. Oncology (Williston Park). 2017. PMID: 28090622 Review.
Cited by
-
Interim FDG PET/CT in primary mediastinal diffuse large B-cell lymphoma: really almost useless procedure?Eur J Nucl Med Mol Imaging. 2018 May;45(5):882-883. doi: 10.1007/s00259-018-3946-y. Epub 2018 Feb 3. Eur J Nucl Med Mol Imaging. 2018. PMID: 29397402 No abstract available.
-
18F-fluorothymidine (FLT)-PET and diffusion-weighted MRI for early response evaluation in patients with small cell lung cancer: a pilot study.Eur J Hybrid Imaging. 2020 Jan 27;4(1):2. doi: 10.1186/s41824-019-0071-5. Eur J Hybrid Imaging. 2020. PMID: 34191195 Free PMC article.
-
FDG-PET/CT in Lymphoma: Where Do We Go Now?Cancers (Basel). 2021 Oct 18;13(20):5222. doi: 10.3390/cancers13205222. Cancers (Basel). 2021. PMID: 34680370 Free PMC article.
-
The value of FDG PET/CT imaging in outcome prediction and response assessment of lymphoma patients treated with immunotherapy: a meta-analysis and systematic review.Eur J Nucl Med Mol Imaging. 2022 Nov;49(13):4661-4676. doi: 10.1007/s00259-022-05918-2. Epub 2022 Aug 6. Eur J Nucl Med Mol Imaging. 2022. PMID: 35932329 Free PMC article.
-
Role of theranostics in thoracic oncology.J Thorac Dis. 2020 Sep;12(9):5140-5146. doi: 10.21037/jtd-2019-pitd-13. J Thorac Dis. 2020. PMID: 33145091 Free PMC article. Review.
References
-
- Cheson BD, Pfistner B, Juweid ME, et al. . Revised response criteria for malignant lymphoma. J Clin Oncol 2007;25(5):579–586. - PubMed
-
- Haioun C, Itti E, Rahmouni A, et al. . [18F]fluoro-2-deoxy-D-glucose positron emission tomography (FDG-PET) in aggressive lymphoma: an early prognostic tool for predicting patient outcome. Blood 2005;106(4):1376–1381. - PubMed
-
- Casasnovas RO, Meignan M, Berriolo-Riedinger A, et al. . SUVmax reduction improves early prognosis value of interim positron emission tomography scans in diffuse large B-cell lymphoma. Blood 2011;118(1):37–43. - PubMed
-
- Römer W, Hanauske AR, Ziegler S, et al. . Positron emission tomography in non-Hodgkin’s lymphoma: assessment of chemotherapy with fluorodeoxyglucose. Blood 1998;91(12):4464–4471. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
