

Immunologic profiles distinguish aviremic HIV-infected adults
- PMID: 26854811
- PMCID: PMC5679214
- DOI: 10.1097/QAD.0000000000001049
Immunologic profiles distinguish aviremic HIV-infected adults
Abstract
Objective: Prior hypothesis-driven studies identified immunophenotypic characteristics associated with the control of HIV replication without antiretroviral therapy (HIV controllers) as well as with the degree of CD4 T-cell recovery during ART. We hypothesized that an unbiased 'discovery-based' approach might identify novel immunologic characteristics of these phenotypes.
Design: We performed immunophenotyping on four 'aviremic' patient groups: HIV controllers (n = 98), antiretroviral-treated immunologic nonresponders (CD4 < 350; n = 59), antiretroviral-treated immunologic responders (CD4 > 350, n = 142), and as a control group HIV-negative adults (n = 43). We measured levels of T-cell maturation, activation, dysfunction, senescence, functionality, and proliferation.
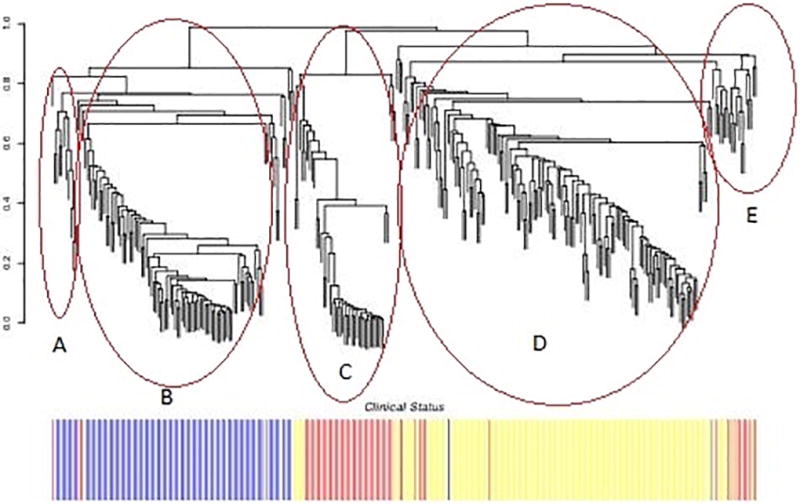
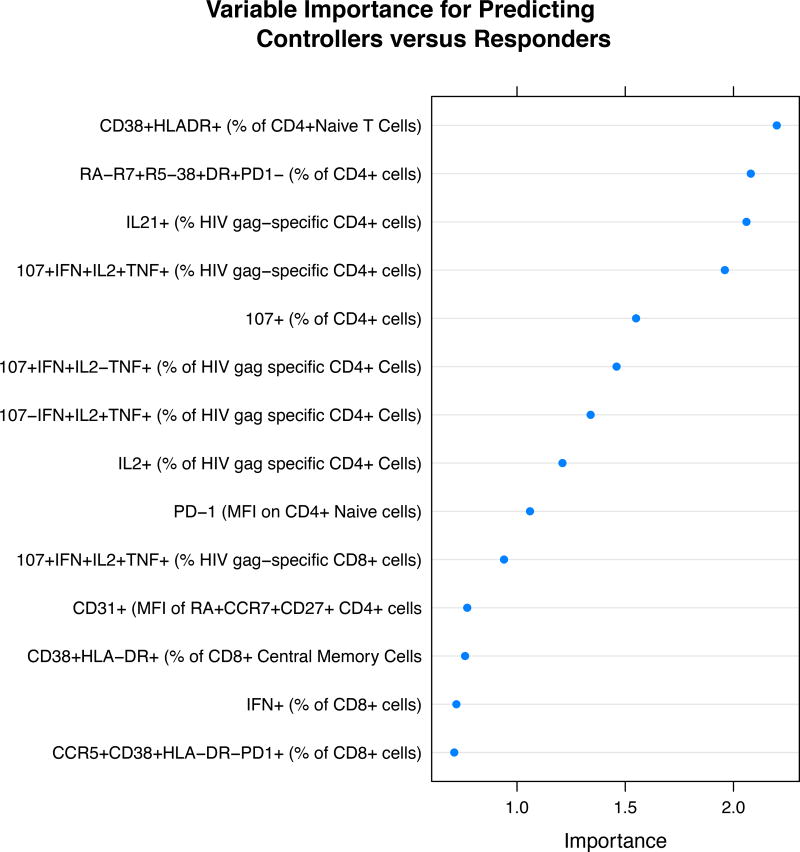
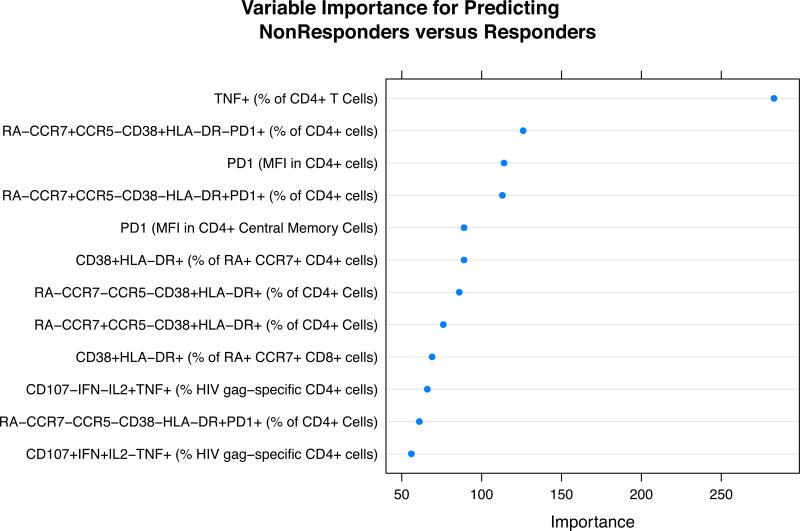
Methods: Supervised learning assessed the relative importance of immune parameters in predicting clinical phenotypes (controller, immunologic responder, or immunologic nonresponder). Unsupervised learning clustered immune parameters and examined if these clusters corresponded to clinical phenotypes.
Results: HIV controllers were characterized by high percentages of HIV-specific T-cell responses and decreased percentages of cells expressing human leukocytic antigen-antigen D related in naive, central memory, and effector T-cell subsets. Immunologic nonresponders were characterized by higher percentages of CD4 T cells that were TNFα+ or INFγ+, higher percentages of activated naive and central memory T cells, and higher percentages of cells expressing programmed cell death protein 1. Unsupervised learning found two distinct clusters of controllers and two distinct clusters of immunologic nonresponders, perhaps suggesting different mechanisms for the clinical outcomes.
Conclusion: Our discovery-based approach confirmed previously reported characteristics that distinguish aviremic individuals, but also identified novel immunologic phenotypes and distinct clinical subpopulations that should lead to more focused pathogenesis studies that might identify targets for novel therapeutic interventions.
Figures
Similar articles
-
CD4+ T cells with an activated and exhausted phenotype distinguish immunodeficiency during aviremic HIV-2 infection.AIDS. 2016 Oct 23;30(16):2415-2426. doi: 10.1097/QAD.0000000000001223. AIDS. 2016. PMID: 27525551 Free PMC article.
-
T-Cell Activation Independently Associates With Immune Senescence in HIV-Infected Recipients of Long-term Antiretroviral Treatment.J Infect Dis. 2016 Jul 15;214(2):216-25. doi: 10.1093/infdis/jiw146. Epub 2016 Apr 12. J Infect Dis. 2016. PMID: 27073222 Free PMC article.
-
HIV-1-infected children on HAART: immunologic features of three different levels of viral suppression.Cytometry B Clin Cytom. 2007 Jan 15;72(1):14-21. doi: 10.1002/cyto.b.20152. Cytometry B Clin Cytom. 2007. PMID: 17041945 Clinical Trial.
-
Specific patterns of CD4-associated immunosenescence in vertically HIV-infected subjects.Clin Microbiol Infect. 2013 Jun;19(6):558-65. doi: 10.1111/j.1469-0691.2012.03934.x. Epub 2012 Jun 27. Clin Microbiol Infect. 2013. PMID: 22735071
-
Immunophenotyping of T cell subpopulations in HIV disease.Curr Protoc Immunol. 2005 Mar;Chapter 12:Unit 12.12. doi: 10.1002/0471142735.im1212s65. Curr Protoc Immunol. 2005. PMID: 18432939 Review.
Cited by
-
Reevaluation of immune activation in the era of cART and an aging HIV-infected population.JCI Insight. 2017 Oct 19;2(20):e95726. doi: 10.1172/jci.insight.95726. JCI Insight. 2017. PMID: 29046481 Free PMC article.
-
PSGL-1, a Strategic Biomarker for Pathological Conditions in HIV Infection: A Hypothesis Review.Viruses. 2023 Oct 31;15(11):2197. doi: 10.3390/v15112197. Viruses. 2023. PMID: 38005875 Free PMC article. Review.
-
Using Machine Learning to Uncover Hidden Heterogeneities in Survey Data.Sci Rep. 2019 Nov 5;9(1):16061. doi: 10.1038/s41598-019-51862-x. Sci Rep. 2019. PMID: 31690743 Free PMC article.
-
Human Immunodeficiency Virus-Infected Immunological Nonresponders Have Colon-Restricted Gut Mucosal Immune Dysfunction.J Infect Dis. 2022 Feb 15;225(4):661-674. doi: 10.1093/infdis/jiaa714. J Infect Dis. 2022. PMID: 33216130 Free PMC article.
-
The Dietary Inflammatory Index Is Not Associated With Gut Permeability or Biomarkers of Systemic Inflammation in HIV Immunologic Non-responders.Front Nutr. 2021 Nov 22;8:736816. doi: 10.3389/fnut.2021.736816. eCollection 2021. Front Nutr. 2021. PMID: 34881278 Free PMC article.
References
-
- Moore RD, Keruly JC. CD4+ cell count 6 years after commencement of highly active antiretroviral therapy in persons with sustained virologic suppression. Clin Infect Dis. 2007;44:441–446. - PubMed
-
- van Lelyveld SF, Gras L, Kesselring A, Zhang S, De Wolf F, Wensing AM, et al. Long-term complications in patients with poor immunological recovery despite virological successful HAART in Dutch ATHENA cohort. AIDS. 2012;26:465–474. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
