

Lipoprotein (a): a Unique Independent Risk Factor for Coronary Artery Disease
- PMID: 26855483
- PMCID: PMC4731365
- DOI: 10.1007/s12291-015-0483-3
Lipoprotein (a): a Unique Independent Risk Factor for Coronary Artery Disease
Abstract
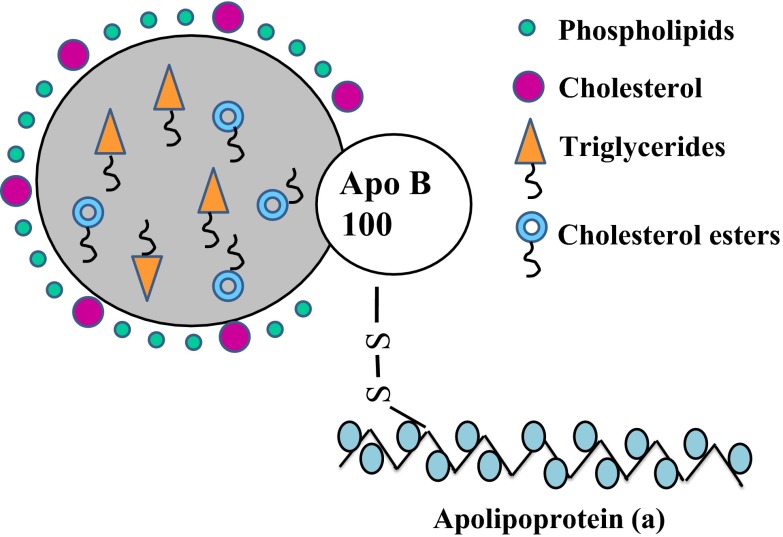
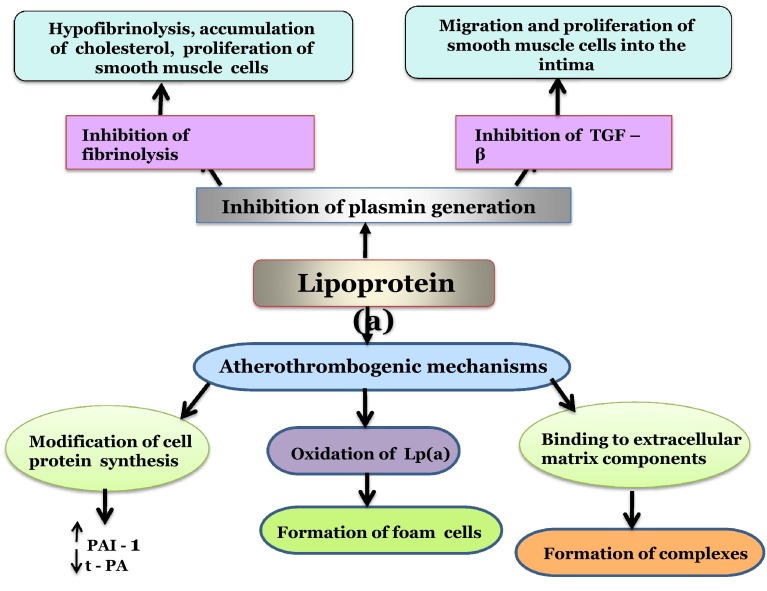
The current epidemic affecting Indians is coronary artery disease (CAD), and is currently one of the most common causes of mortality and morbidity in developed and developing countries. The higher rate of CAD in Indians, as compared to people of other ethnic origin, may indicate a possible genetic susceptibility. Hence, Lp(a), an independent genetic risk marker for atherosclerosis and cardiovascular disease assumes great importance. Lp(a), an atherogenic lipoprotein, contains a cholesterol rich LDL particle, one molecule of apolipoprotein B-100 and a unique protein, apolipoprotein (a) which distinguishes it from LDL. Apo(a) is highly polymorphic and an inverse relationship between Lp(a) concentration and apo(a) isoform size has been observed. This is genetically controlled suggesting a functional diversity among the apo(a) isoforms. The LPA gene codes for apo(a) whose genetic heterogeneity is due to variations in its number of kringles. The exact pathogenic mechanism of Lp(a) is still not completely elucidated, but the structural homology of Lp(a) with LDL and plasmin is possibly responsible for its acting as a link between atherosclerosis and thrombosis. Upper limits of normal Lp(a) levels have not been defined for the Indian population. A cut off limit of 20 mg/dL has been suggested while for the Caucasian population it is 30 mg/dL. Though a variety of assays are available for its measurement, standardization of the analytical method is highly complicated as a majority of the methods are affected by the heterogeneity in apo(a) size. No therapeutic drug selectively targets Lp(a) but recently, new modifiers of apo(a) synthesis are being considered.
Keywords: Apolipoprotein (a); Coronary artery disease; Genetics; Lipoprotein (a); Risk factor.
Figures
Similar articles
-
Lipoprotein(a) as a risk factor for coronary artery disease.Am J Cardiol. 1998 Dec 17;82(12A):57U-66U; discussion 86U. doi: 10.1016/s0002-9149(98)00954-0. Am J Cardiol. 1998. PMID: 9915664 Review.
-
Correlation of lipoprotein (a) to angiographically defined coronary artery disease in Indians.Int J Cardiol. 1996 Dec 13;57(3):265-70. doi: 10.1016/s0167-5273(96)02800-8. Int J Cardiol. 1996. PMID: 9024915
-
Genomic structure and organization of kringles type 3 to 10 of the apolipoprotein(a) gene in 6q26-27.Gene. 1997 Sep 1;196(1-2):1-8. doi: 10.1016/s0378-1119(97)00091-7. Gene. 1997. PMID: 9322734
-
Lipoprotein(a) and apolipoprotein(a) isoform size: Associations with angiographic extent and severity of coronary artery disease, and carotid artery plaque.Atherosclerosis. 2018 Aug;275:232-238. doi: 10.1016/j.atherosclerosis.2018.06.863. Epub 2018 Jun 18. Atherosclerosis. 2018. PMID: 29960898
-
Lipoprotein(a) metabolism: potential sites for therapeutic targets.Metabolism. 2013 Apr;62(4):479-91. doi: 10.1016/j.metabol.2012.07.024. Epub 2012 Oct 4. Metabolism. 2013. PMID: 23040268 Free PMC article. Review.
Cited by
-
Analysis of traditional and emerging risk factors in premenopausal women with coronary artery disease: A pilot-scale study from North India.Mol Cell Biochem. 2017 Aug;432(1-2):67-78. doi: 10.1007/s11010-017-2998-9. Epub 2017 Mar 23. Mol Cell Biochem. 2017. PMID: 28337704 Clinical Trial.
-
High Lipoprotein(a) Levels as a Predictor of Major Adverse Cardiovascular Events in Hospitalized-Acute Myocardial Infarction Patients.Vasc Health Risk Manag. 2020 Apr 8;16:125-132. doi: 10.2147/VHRM.S233503. eCollection 2020. Vasc Health Risk Manag. 2020. PMID: 32308405 Free PMC article.
-
Evaluation of lipoprotein (a) [Lp(a)] and lipid abnormalities in patients with newly detected hypertension and its association with severity of hypertension.J Family Med Prim Care. 2022 Apr;11(4):1508-1513. doi: 10.4103/jfmpc.jfmpc_989_21. Epub 2022 Mar 18. J Family Med Prim Care. 2022. PMID: 35516713 Free PMC article.
-
Lipoprotein (a) level as a risk factor for stroke and its subtype: A systematic review and meta-analysis.Sci Rep. 2021 Aug 2;11(1):15660. doi: 10.1038/s41598-021-95141-0. Sci Rep. 2021. PMID: 34341405 Free PMC article.
-
Effects of blood lipid stability on progression of carotid atherosclerosis.Pak J Med Sci. 2017 May-Jun;33(3):599-602. doi: 10.12669/pjms.333.12593. Pak J Med Sci. 2017. PMID: 28811778 Free PMC article.
References
-
- Bulatao RA, Stephens PW. Global estimates and projections of mortality by cause, 1970–2015. Preworking paper 1007. Washington: Population and Nutrition Department, World Bank 1992.
-
- Enas EA, Yusuf S, Mehta J. Meeting of international working group on coronary artery disease in South Asians. Indian Heart J. 1996;48:727–732. - PubMed
-
- Rissam HS, Kishore S, Trehan N. Coronary artery disease in young Indians—the missing link. J Indian Acad Clin Med. 2001;2(3):128–131.
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous