

Effectiveness and safety of continuous wound infiltration for postoperative pain management after open gastrectomy
- PMID: 26855550
- PMCID: PMC4724622
- DOI: 10.3748/wjg.v22.i5.1902
Effectiveness and safety of continuous wound infiltration for postoperative pain management after open gastrectomy
Abstract
Aim: To prospectively evaluate the effectiveness and safety of continuous wound infiltration (CWI) for pain management after open gastrectomy.
Methods: Seventy-five adult patients with American Society of Anesthesiologists (ASA) Physical Status Classification System (ASA) grade 1-3 undergoing open gastrectomy were randomized to three groups. Group 1 patients received CWI with 0.3% ropivacaine (group CWI). Group 2 patients received 0.5 mg/mL morphine intravenously by a patient-controlled analgesia pump (PCIA) (group PCIA). Group 3 patients received epidural analgesia (EA) with 0.12% ropivacaine and 20 µg/mL morphine with an infusion at 6-8 mL/h for 48 h (group EA). A standard general anesthetic technique was used for all three groups. Rescue analgesia (2 mg bolus of morphine, intravenous) was given when the visual analogue scale (VAS) score was ≥ 4. The outcomes measured over 48 h after the operation were VAS scores both at rest and during mobilization, total morphine consumption, relative side effects, and basic vital signs. Further results including time to extubation, recovery of bowel function, surgical wound healing, mean length of hospitalization after surgery, and the patient's satisfaction were also recorded.
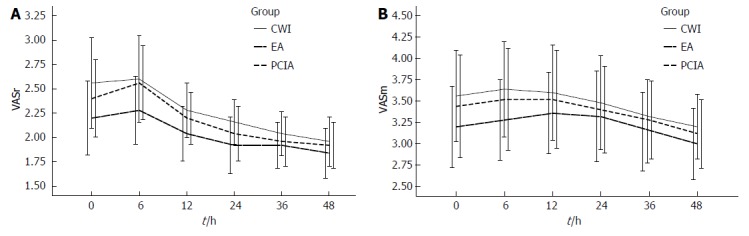
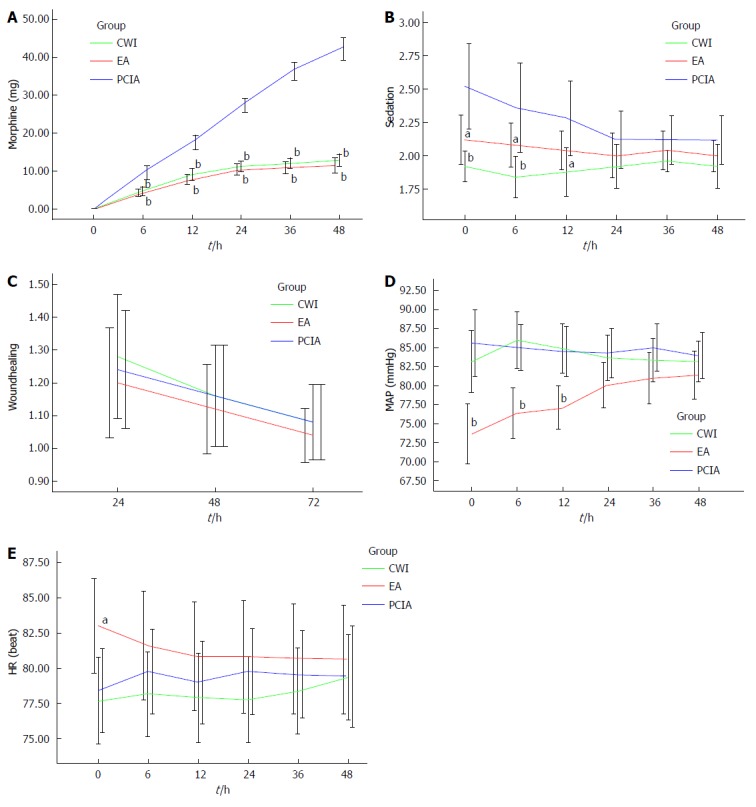
Results: All three groups had similar VAS scores during the first 48 h after surgery. Group CWI and group EA, compared with group PCIA, had lower morphine consumption (P < 0.001), less postoperative nausea and vomiting (1.20 ± 0.41 vs 1.96 ± 0.67, 1.32 ± 0.56 vs 1.96 ± 0.67, respectively, P < 0.001), earlier extubation (16.56 ± 5.24 min vs 19.76 ± 5.75 min, P < 0.05, 15.48 ± 4.59 min vs 19.76 ± 5.75 min, P < 0.01), and earlier recovery of bowel function (2.96 ± 1.17 d vs 3.60 ± 1.04 d, 2.80 ± 1.38 d vs 3.60 ± 1.04 d, respectively, P < 0.05). The mean length of hospitalization after surgery was reduced in groups CWI (8.20 ± 2.58 d vs 10.08 ± 3.15 d, P < 0.05) and EA (7.96 ± 2.30 d vs 10.08 ± 3.15 d, P < 0.01) compared with group PCIA. All three groups had similar patient satisfaction and wound healing, but group PCIA was prone to higher sedation scores when compared with groups CWI and EA, especially during the first 12 h after surgery. Group EA had a lower mean arterial pressure within the first postoperative 12 h compared with the other two groups.
Conclusion: CWI with ropivacaine yields a satisfactory analgesic effect within the first 48 h after open gastrectomy, with lower morphine consumption and accelerated recovery.
Keywords: Epidural analgesia; Gastrectomy; Incision infection; Patient-controlled analgesia; Postoperative pain; Ropivacaine; Wound infiltration.
Figures
Similar articles
-
The analgesic efficacy of subcostal transversus abdominis plane block compared with thoracic epidural analgesia and intravenous opioid analgesia after radical gastrectomy.Anesth Analg. 2013 Aug;117(2):507-13. doi: 10.1213/ANE.0b013e318297fcee. Epub 2013 Jun 6. Anesth Analg. 2013. PMID: 23744953 Clinical Trial.
-
The postoperative analgesic efficacy of preperitoneal continuous wound infusion compared to epidural continuous infusion with local anesthetics after colorectal cancer surgery: a randomized controlled multicenter study.Anesth Analg. 2012 Dec;115(6):1442-50. doi: 10.1213/ANE.0b013e31826b4694. Epub 2012 Nov 9. Anesth Analg. 2012. PMID: 23144438 Clinical Trial.
-
Effectiveness of Epidural Analgesia, Continuous Surgical Site Analgesia, and Patient-Controlled Analgesic Morphine for Postoperative Pain Management and Hyperalgesia, Rehabilitation, and Health-Related Quality of Life After Open Nephrectomy: A Prospective, Randomized, Controlled Study.Anesth Analg. 2017 Jan;124(1):336-345. doi: 10.1213/ANE.0000000000001688. Anesth Analg. 2017. PMID: 27918333 Clinical Trial.
-
Intra-operative paravertebral block for postoperative analgesia in thoracotomy patients: a randomized, double-blind, placebo-controlled study.Eur J Cardiothorac Surg. 2011 Oct;40(4):902-6. doi: 10.1016/j.ejcts.2011.01.067. Epub 2011 Mar 5. Eur J Cardiothorac Surg. 2011. PMID: 21377888 Review.
-
Epidural Local Anesthetics Versus Opioid-Based Analgesic Regimens for Postoperative Gastrointestinal Paralysis, Vomiting, and Pain After Abdominal Surgery: A Cochrane Review.Anesth Analg. 2016 Dec;123(6):1591-1602. doi: 10.1213/ANE.0000000000001628. Anesth Analg. 2016. PMID: 27870743 Review.
Cited by
-
Optimizing postoperative pain management in minimally invasive colorectal surgery.Ann Coloproctol. 2024 Dec;40(6):525-526. doi: 10.3393/ac.2024.00815.0116. Epub 2024 Dec 3. Ann Coloproctol. 2024. PMID: 39623936 Free PMC article. No abstract available.
-
To assess the analgesic efficacy of adjuvant magnesium sulfate added with ropivacaine over ropivacaine alone as a continuous infiltration in total abdominal hysterectomy wound: A randomized controlled trial.J Anaesthesiol Clin Pharmacol. 2024 Jan-Mar;40(1):140-146. doi: 10.4103/joacp.joacp_239_22. Epub 2024 Mar 14. J Anaesthesiol Clin Pharmacol. 2024. PMID: 38666179 Free PMC article.
-
Use of local wound infiltration in open hepatectomy to reduce wound pain: A systematic review and meta-analysis.Int Wound J. 2023 Nov;20(9):3760-3767. doi: 10.1111/iwj.14271. Epub 2023 Jun 7. Int Wound J. 2023. Retraction in: Int Wound J. 2025 Mar;22(3):e70305. doi: 10.1111/iwj.70305. PMID: 37287429 Free PMC article. Retracted.
-
Effects of dexmedetomidine in combination with fentanyl-based intravenous patient-controlled analgesia on pain attenuation after open gastrectomy in comparison with conventional thoracic epidural and fentanyl-based intravenous patient-controlled analgesia.Int J Med Sci. 2017 Aug 18;14(10):951-960. doi: 10.7150/ijms.20347. eCollection 2017. Int J Med Sci. 2017. PMID: 28924366 Free PMC article. Clinical Trial.
-
A prospective cohort study on perioperative percutaneous balloon compression for trigeminal neuralgia: safety and efficacy analysis.Neurosurg Rev. 2024 Feb 17;47(1):86. doi: 10.1007/s10143-024-02323-1. Neurosurg Rev. 2024. PMID: 38366200
References
-
- Dajczman E, Gordon A, Kreisman H, Wolkove N. Long-term postthoracotomy pain. Chest. 1991;99:270–274. - PubMed
-
- Wightman JA. A prospective survey of the incidence of postoperative pulmonary complications. Br J Surg. 1968;55:85–91. - PubMed
-
- Latimer RG, Dickman M, Day WC, Gunn ML, Schmidt CD. Ventilatory patterns and pulmonary complications after upper abdominal surgery determined by preoperative and postoperative computerized spirometry and blood gas analysis. Am J Surg. 1971;122:622–632. - PubMed
-
- Young A, Buvanendran A. Recent advances in multimodal analgesia. Anesthesiol Clin. 2012;30:91–100. - PubMed
-
- Elvir-Lazo OL, White PF. Postoperative pain management after ambulatory surgery: role of multimodal analgesia. Anesthesiol Clin. 2010;28:217–224. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
