

Anteroposterior Radiographs Are More Accurate than Cross-Table Lateral Radiographs for Acetabular Anteversion Assessment: a Retrospective Cohort Study
- PMID: 26855625
- PMCID: PMC4733699
- DOI: 10.1007/s11420-015-9472-6
Anteroposterior Radiographs Are More Accurate than Cross-Table Lateral Radiographs for Acetabular Anteversion Assessment: a Retrospective Cohort Study
Abstract
Background: Measuring acetabular anteversion is relevant to routine follow-up of total hip arthroplasties (THAs) and for malfunctioning THAs. Imageless navigation facilitates acetabular component orientation relative to the anterior pelvic plane (APP) or to the APP adjusted for sagittal pelvic tilt (PT). The optimal plain radiographic method for the postoperative assessment of anteversion is not agreed upon.
Questions/purposes: (1) Do anteversion measurements on plain radiographs correlate more with APP anteversion or PT-adjusted anteversion? (2) Do measurements of anteversion performed on supine anteroposterior (AP) radiographs more accurately reflect intraoperative anteversion values for navigated THA compared to anteversion measured on cross-table lateral (CL) radiographs?
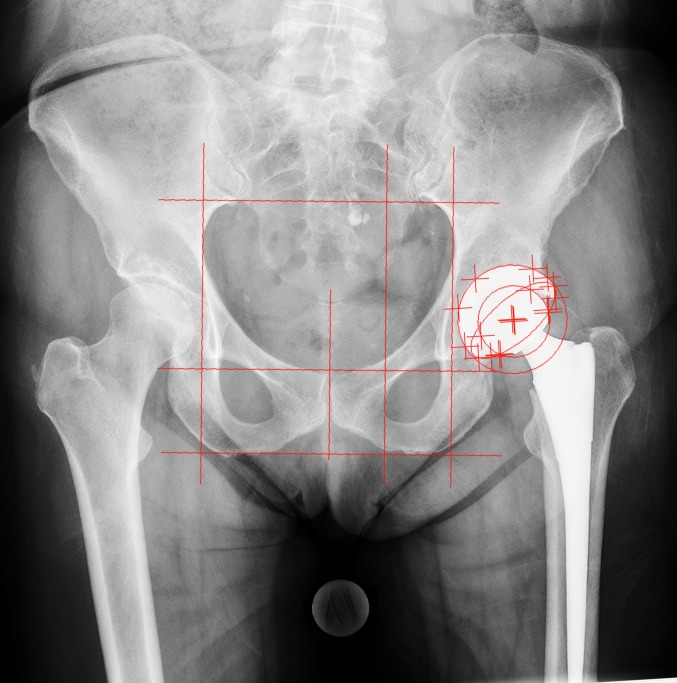
Methods: Seventy patients receiving primary navigated THA were included. APP and PT-adjusted anteversion were recorded; the latter defined the intraoperative target for anteversion. Postoperative anteversion was measured on supine AP pelvis radiographs with computer software and CL radiographs with conventional methods. Intraoperative measurements were used as the reference standards for comparisons.
Results: Mean intraoperative APP anteversion was 20.6° ± 5.6°. Mean intraoperative PT-adjusted anteversion was 22.9° ± 4.5°. Mean anteversion was 22.7° ± 4.7° on AP radiographs and 27.2° ± 4.2° on CL radiographs (p < 0.001). Only correlations between PT-adjusted anteversion and radiographic assessments of anteversion were significant. The mean difference between PT-adjusted anteversion and anteversion on AP radiographs was -0.2° ± 4.3°, while the mean difference between the PT-adjusted anteversion and anteversion measured on CL radiographs was 4.3 ± 5.1° (p < 0.001).
Conclusion: Plain film assessment of anteversion was more accurate on supine AP radiographs than on CL radiographs, which overestimated acetabular anteversion.
Keywords: anteversion; computer-assisted surgery; diagnostic imaging; radiographic film; total hip replacement.
Figures

References
-
- Barrack RL. Dislocation after total hip arthroplasty: implant design and orientation. J Am Acad Orthop Surg. 2003;11(2):89–99. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
