

Use of venous-to-arterial carbon dioxide tension difference to guide resuscitation therapy in septic shock
- PMID: 26855893
- PMCID: PMC4733455
- DOI: 10.5492/wjccm.v5.i1.47
Use of venous-to-arterial carbon dioxide tension difference to guide resuscitation therapy in septic shock
Abstract
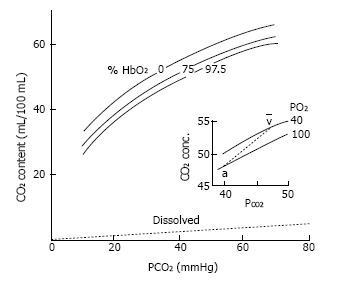
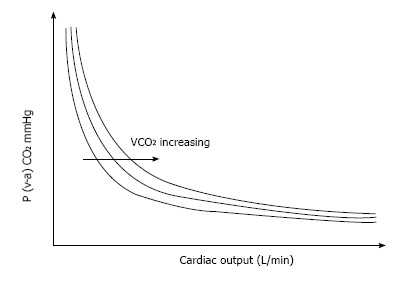
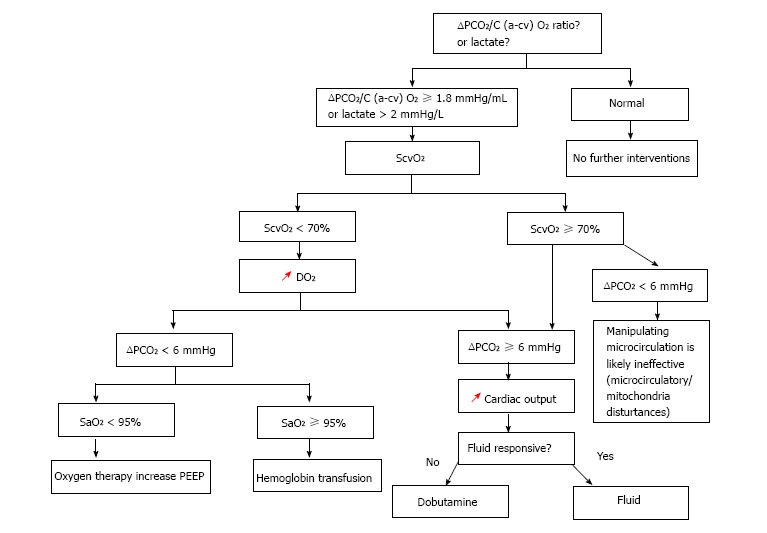
The mixed venous-to-arterial carbon dioxide (CO2) tension difference [P (v-a) CO2] is the difference between carbon dioxide tension (PCO2) in mixed venous blood (sampled from a pulmonary artery catheter) and the PCO2 in arterial blood. P (v-a) CO2 depends on the cardiac output and the global CO2 production, and on the complex relationship between PCO2 and CO2 content. Experimental and clinical studies support the evidence that P (v-a) CO2 cannot serve as an indicator of tissue hypoxia, and should be regarded as an indicator of the adequacy of venous blood to wash out the total CO2 generated by the peripheral tissues. P (v-a) CO2 can be replaced by the central venous-to-arterial CO2 difference (ΔPCO2), which is calculated from simultaneous sampling of central venous blood from a central vein catheter and arterial blood and, therefore, more easy to obtain at the bedside. Determining the ΔPCO2 during the resuscitation of septic shock patients might be useful when deciding when to continue resuscitation despite a central venous oxygen saturation (ScvO2) > 70% associated with elevated blood lactate levels. Because high blood lactate levels is not a discriminatory factor in determining the source of that stress, an increased ΔPCO2 (> 6 mmHg) could be used to identify patients who still remain inadequately resuscitated. Monitoring the ΔPCO2 from the beginning of the reanimation of septic shock patients might be a valuable means to evaluate the adequacy of cardiac output in tissue perfusion and, thus, guiding the therapy. In this respect, it can aid to titrate inotropes to adjust oxygen delivery to CO2 production, or to choose between hemoglobin correction or fluid/inotrope infusion in patients with a too low ScvO2 related to metabolic demand. The combination of P (v-a) CO2 or ΔPCO2 with oxygen-derived parameters through the calculation of the P (v-a) CO2 or ΔPCO2/arteriovenous oxygen content difference ratio can detect the presence of global anaerobic metabolism.
Keywords: Anaerobic metabolism; Carbon dioxide production; Cardiac output; Oxygen consumption; Oxygen supply dependency; Resuscitation; Septic shock; Venous-to-arterial carbon dioxide tension difference; tissue hypoxia.
Figures
References
-
- Krafft P, Steltzer H, Hiesmayr M, Klimscha W, Hammerle AF. Mixed venous oxygen saturation in critically ill septic shock patients. The role of defined events. Chest. 1993;103:900–906. - PubMed
-
- Schumacker PT, Cain SM. The concept of a critical oxygen delivery. Intensive Care Med. 1987;13:223–229. - PubMed
-
- Nelson DP, Samsel RW, Wood LD, Schumacker PT. Pathological supply dependence of systemic and intestinal O2 uptake during endotoxemia. J Appl Physiol (1985) 1988;64:2410–2419. - PubMed
-
- Zhang H, Vincent JL. Oxygen extraction is altered by endotoxin during tamponade-induced stagnant hypoxia in the dog. Circ Shock. 1993;40:168–176. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
