

Prognostic factors associated with hospital survival in comatose survivors of cardiac arrest
- PMID: 26855900
- PMCID: PMC4733450
- DOI: 10.5492/wjccm.v5.i1.103
Prognostic factors associated with hospital survival in comatose survivors of cardiac arrest
Abstract
Aim: To identify patient, cardiac arrest and management factors associated with hospital survival in comatose survivors of cardiac arrest.
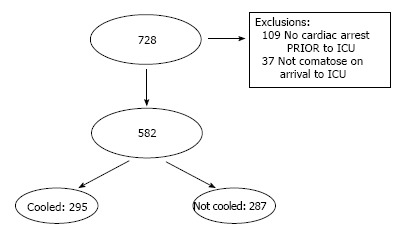
Methods: A retrospective, single centre study of comatose patients admitted to our intensive care unit (ICU) following cardiac arrest during the twenty year period between 1993 and 2012. This study was deemed by the Human Research Ethics Committee (HREC) of Monash Health to be a quality assurance exercise, and thus did not require submission to the Monash Health HREC (Research Project Application, No. 13290Q). The study population included all patients admitted to our ICU between 1993 and 2012, with a discharge diagnosis including "cardiac arrest". Patients were excluded if they did not have a cardiac arrest prior to ICU admission (i.e., if their primary arrest was during their admission to ICU), or were not comatose on arrival to ICU. Our primary outcome measure was survival to hospital discharge. Secondary outcome measures were ICU and hospital length of stay (LOS), and factors associated with survival to hospital discharge.
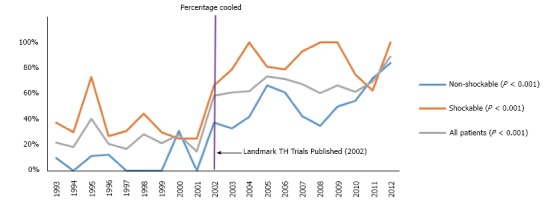
Results: Five hundred and eighty-two comatose patients were admitted to our ICU following cardiac arrest, with 35% surviving to hospital discharge. The median ICU and hospital LOS was 3 and 5 d respectively. There was no survival difference between in-hospital and out-of-hospital cardiac arrests. Males made up 62% of our cardiac arrest population, were more likely to have a shockable rhythm (56% vs 37%, P < 0.001), and were more likely to survive to hospital discharge (40% vs 28%, P = 0.006). On univariate analysis, therapeutic hypothermia, regardless of method used (e.g., rapid infusion of ice cold fluids, topical ice, "Arctic Sun", passive rewarming, "Bair Hugger") and location initiated (e.g., pre-hospital, emergency department, intensive care) was associated with increased survival. There was however no difference in survival associated with target temperature, time at target temperature, location of initial cooling, method of initiating cooling, method of maintaining cooling or method of rewarming. Patients that survived were more likely to have a shockable rhythm (P < 0.001), shorter time to return of spontaneous circulation (P < 0.001), receive therapeutic hypothermia (P = 0.03), be of male gender (P = 0.006) and have a lower APACHE II score (P < 0.001). After multivariate analysis, only a shockable initial rhythm (OR = 6.4, 95%CI: 3.95-10.4; P < 0.01) and a shorter time to return of spontaneous circulation (OR = 0.95, 95%CI: 0.93-0.97; P < 0.01) was found to be independently associated with survival to hospital discharge.
Conclusion: In comatose survivors of cardiac arrest, shockable rhythm and shorter time to return of spontaneous circulation were independently associated with increased survival to hospital discharge.
Keywords: Arrhythmia; Cardiac arrest; Hyperthermia; Hypothermia; Resuscitation.
Figures
Similar articles
-
Impact of Induced Therapeutic Hypothermia by Intravenous Infusion of Ice-Cold Fluids After Hospital Arrival in Comatose Survivors of Out-of-Hospital Cardiac Arrest With Initial Shockable Rhythm.Circ J. 2021 Sep 24;85(10):1842-1848. doi: 10.1253/circj.CJ-20-0793. Epub 2021 Jul 14. Circ J. 2021. PMID: 34261843
-
Impact of presenting rhythm on short- and long-term neurologic outcome in comatose survivors of cardiac arrest treated with therapeutic hypothermia.Crit Care Med. 2014 Oct;42(10):2225-34. doi: 10.1097/CCM.0000000000000506. Crit Care Med. 2014. PMID: 25014063 Free PMC article.
-
Esophageal temperature after out-of-hospital cardiac arrest: an observational study.Resuscitation. 2010 Jul;81(7):867-71. doi: 10.1016/j.resuscitation.2010.03.017. Epub 2010 Apr 21. Resuscitation. 2010. PMID: 20413203
-
Targeted Temperature Management in Cardiac Arrest: An Updated Narrative Review.Cardiol Ther. 2023 Mar;12(1):65-84. doi: 10.1007/s40119-022-00292-4. Epub 2022 Dec 17. Cardiol Ther. 2023. PMID: 36527676 Free PMC article. Review.
-
Beyond return of spontaneous circulation: update on post-cardiac arrest management in the intensive care unit.Singapore Med J. 2021 Aug;62(8):444-451. doi: 10.11622/smedj.2021115. Singapore Med J. 2021. PMID: 35001117 Free PMC article. Review.
Cited by
-
Association of Hypercapnia and Hypercapnic Acidosis With Clinical Outcomes in Mechanically Ventilated Patients With Cerebral Injury.JAMA Neurol. 2018 Jul 1;75(7):818-826. doi: 10.1001/jamaneurol.2018.0123. JAMA Neurol. 2018. PMID: 29554187 Free PMC article.
-
Clinical outcomes of 3-year experience of targeted temperature management in patients with out-of-hospital cardiac arrest at Songklanagarind Hospital in Southern Thailand: an analysis of the MICU-TTM registry.Open Access Emerg Med. 2016 Sep 6;8:67-72. doi: 10.2147/OAEM.S113214. eCollection 2016. Open Access Emerg Med. 2016. PMID: 27660500 Free PMC article.
References
-
- Jennings PA, Cameron P, Walker T, Bernard S, Smith K. Out-of-hospital cardiac arrest in Victoria: rural and urban outcomes. Med J Aust. 2006;185:135–139. - PubMed
-
- Bernard S. Outcome from prehospital cardiac arrest in Melbourne, Australia. Emerg Med. 1998;10:25–29.
-
- Hypothermia after Cardiac Arrest Study Group. Mild therapeutic hypothermia to improve the neurologic outcome after cardiac arrest. N Engl J Med. 2002;346:549–556. - PubMed
-
- Nielsen N, Wetterslev J, Cronberg T, Erlinge D, Gasche Y, Hassager C, Horn J, Hovdenes J, Kjaergaard J, Kuiper M, et al. Targeted temperature management at 33°C versus 36°C after cardiac arrest. N Engl J Med. 2013;369:2197–2206. - PubMed
-
- Lin S, Scales DC, Dorian P, Kiss A, Common MR, Brooks SC, Goodman SG, Salciccioli JD, Morrison LJ. Targeted temperature management processes and outcomes after out-of-hospital cardiac arrest: an observational cohort study*. Crit Care Med. 2014;42:2565–2574. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
