

Communicating Tubular Esophageal Duplication Combined with Bronchoesophageal Fistula
- PMID: 26855929
- PMCID: PMC4743716
- DOI: 10.5946/ce.2016.49.1.81
Communicating Tubular Esophageal Duplication Combined with Bronchoesophageal Fistula
Abstract
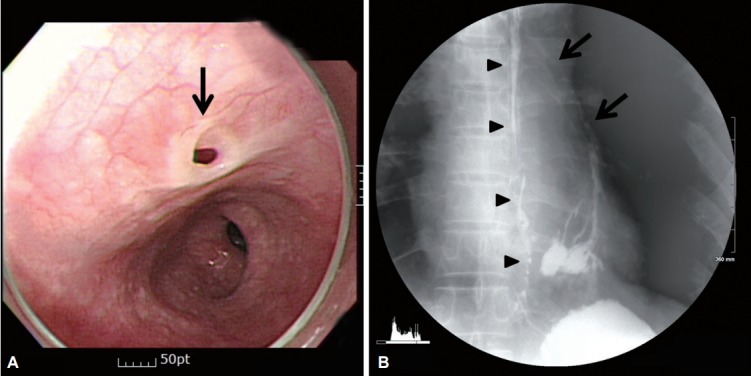
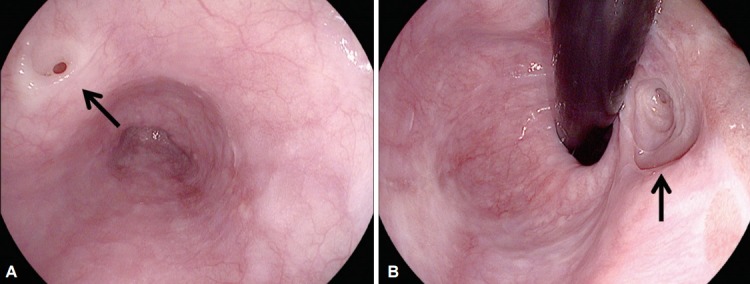
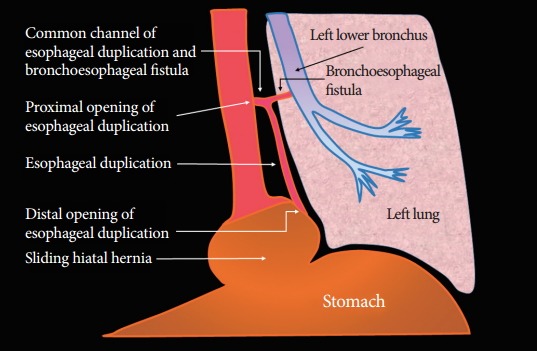
Esophageal duplication (ED) is rarely diagnosed in adults and is usually asymptomatic. Especially, ED that is connected to the esophagus through a tubular communication and combined with bronchoesophageal fistula (BEF) is extremely rare and has never been reported in the English literature. This condition is very difficult to diagnose. Although some combinations of several modalities, such as upper gastrointestinal endoscopy, esophagography, computed tomography, magnetic resonance imaging, and endoscopic ultrasonography, can be used for the diagnosis, the results might be inconclusive. Here, we report on a patient with communicating tubular ED that was incidentally diagnosed on the basis of endoscopy and esophagography during the postoperational evaluation of BEF.
Keywords: Bronchial fistula; Bronchoesophageal fistula; Esophageal duplication; Esophageal fistula.
Conflict of interest statement
Figures


Similar articles
-
[Esophageal duplication with esophago-bronchial fistula].Nihon Kyobu Geka Gakkai Zasshi. 1994 Feb;42(2):286-91. Nihon Kyobu Geka Gakkai Zasshi. 1994. PMID: 8138702 Review. Japanese.
-
Esophageal bypass surgery as a definitive repair of recurrent acquired benign bronchoesophageal fistula.J Cardiothorac Surg. 2019 Apr 11;14(1):73. doi: 10.1186/s13019-019-0902-2. J Cardiothorac Surg. 2019. PMID: 30971283 Free PMC article.
-
Endoscopic submucosal dissection-based suture combined with medical adhesive for complicated tuberculous bronchoesophageal fistula: a case report.J Int Med Res. 2022 Feb;50(2):3000605221080723. doi: 10.1177/03000605221080723. J Int Med Res. 2022. PMID: 35225721 Free PMC article.
-
A rare case of congenital bronchoesophageal fistula in an adult.Int J Surg Case Rep. 2017;36:182-184. doi: 10.1016/j.ijscr.2017.03.029. Epub 2017 Mar 21. Int J Surg Case Rep. 2017. PMID: 28442319 Free PMC article.
-
Canine bronchoesophageal fistulas: case report and literature review.Compend Contin Educ Vet. 2010 Apr;32(4):E1. Compend Contin Educ Vet. 2010. PMID: 20949418 Review.
Cited by
-
Endoscopic management of a tubular esophageal duplication in a young adult.VideoGIE. 2020 Jun 29;5(10):455-457. doi: 10.1016/j.vgie.2020.05.013. eCollection 2020 Oct. VideoGIE. 2020. PMID: 33102995 Free PMC article. No abstract available.
-
Tubular Duplication of the Esophagus in a Newborn, Treated by Thoracoscopy.European J Pediatr Surg Rep. 2022 Mar 10;10(1):e49-e52. doi: 10.1055/s-0042-1742594. eCollection 2022 Jan. European J Pediatr Surg Rep. 2022. PMID: 35282300 Free PMC article.
-
Endoscopic septum division of tubular esophageal duplication in two children and systematic review.Pediatr Surg Int. 2022 Nov;38(11):1525-1531. doi: 10.1007/s00383-022-05205-z. Epub 2022 Sep 1. Pediatr Surg Int. 2022. PMID: 36048241
References
-
- Arbona JL, Fazzi JG, Mayoral J. Congenital esophageal cysts: case report and review of literature. Am J Gastroenterol. 1984;79:177–182. - PubMed
-
- Phadke AY, Shah SK, Rajput SL, Bhandarkar PV, Abraham P. Incomplete tubular duplication of the esophagus lined by heterotopic gastric epithelium, presenting in adulthood. Endoscopy. 2000;32:S35–S36. - PubMed
-
- Kumar D, Samujh R, Rao KL. Infected esophageal duplication cyst simulating empyema. Indian Pediatr. 2003;40:423–425. - PubMed
-
- Bagheri R, Asnaashari AM, Afghani R. Esophageal duplication cyst. Asian Cardiovasc Thorac Ann. 2015;23:332–334. - PubMed
-
- Kiratli PO, Aksoy T, Bozkurt MF, Orhan D. Detection of ectopic gastric mucosa using 99mTc pertechnetate: review of the literature. Ann Nucl Med. 2009;23:97–105. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
