

Inequality and inequity in healthcare utilization in urban Nepal: a cross-sectional observational study
- PMID: 26856362
- PMCID: PMC4977425
- DOI: 10.1093/heapol/czv137
Inequality and inequity in healthcare utilization in urban Nepal: a cross-sectional observational study
Abstract
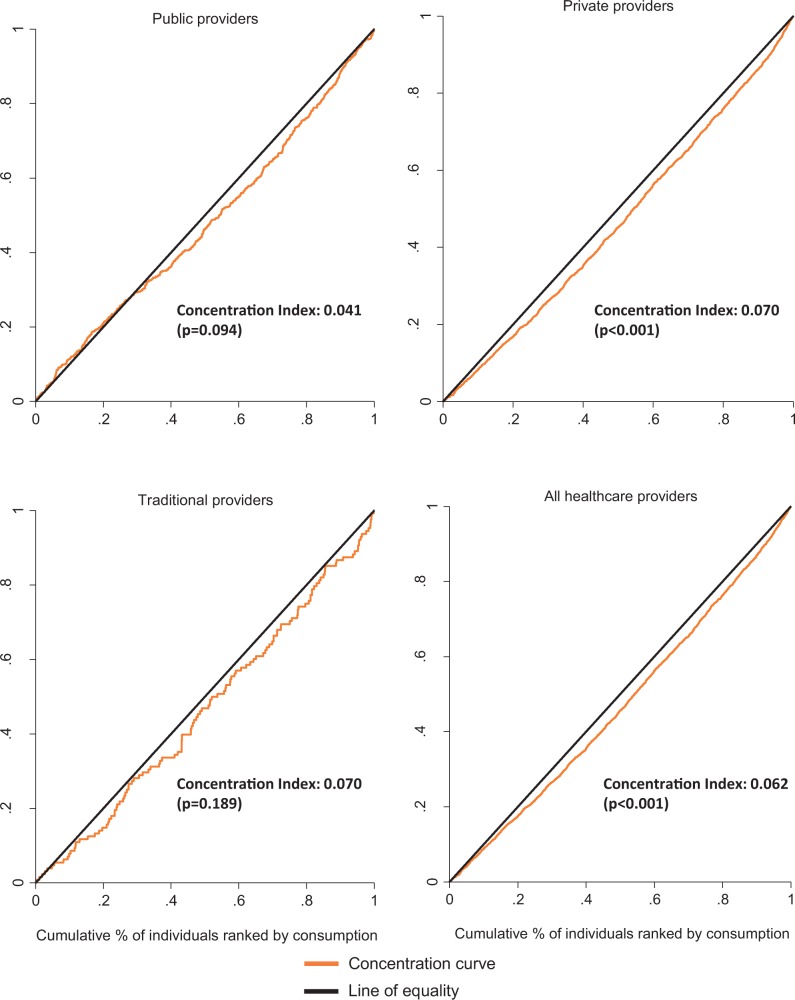
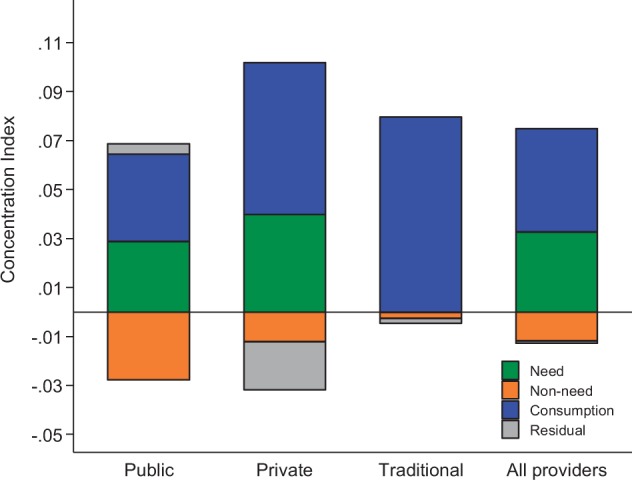
Inequality in access to quality healthcare is a major health policy challenge in many low- and middle-income countries. This study aimed to identify the major sources of inequity in healthcare utilization using a population-based household survey from urban Nepal. A cross-sectional survey was conducted covering 9177 individuals residing in 1997 households in five municipalities of Kathmandu valley between 2011 and 2012. The concentration index was calculated and a decomposition method was used to measure inequality in healthcare utilization, along with a horizontal inequity index (HI) to estimate socioeconomic inequalities in healthcare utilization. Results showed a significant pro-rich distribution of general healthcare utilization in all service providers (Concentration Index: 0.062, P < 0.001; HI: 0.029, P < 0.05) and private service providers (Concentration Index: 0.070, P < 0.001; HI: 0.030, P < 0.05). The pro-rich distribution of probability in general healthcare utilization was attributable to inequalities in the level of household economic status (percentage contribution: 67.8%) and in the self-reported prevalence of non-communicable diseases such as hypertension (36.7%) and diabetes (14.4%). Despite the provision of free services by public healthcare providers, our analysis found no evidence of the poor making more use of public health services (Concentration Index: 0.041, P = 0.094). Interventions to reduce the household economic burden of major illnesses, coupled with improvement in the management of public health facilities, warrant further attention by policy-makers.
Keywords: : Health economics; health care utilization; health inequalities.
© The Author 2016. Published by Oxford University Press in association with The London School of Hygiene and Tropical Medicine.
Figures
References
-
- Bago d’Uva T, Jones AM, Van Doorslaer E. 2009. Measurement of horizontal inequity in health care utilisation using European panel data. Journal of Health Economics 28: 280–289. - PubMed
-
- Belay T, Tandon A. 2011. Assessing fiscal space for health in Nepal. Heath, nutrition and population discussion paper. Washington, DC: World Bank; http://documents.worldbank.org/curated/en/2011/07/16240700/assessing-fis..., accessed 25 July 2012.
-
- Bonfrer I, Van De Poel E, Grimm M, Van Doorslaer E. 2014. Does the distribution of healthcare utilization match needs in Africa? Health Policy and Planning 29: 921–937. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
