

Comparing Luminex NxTAG-Respiratory Pathogen Panel and RespiFinder-22 for multiplex detection of respiratory pathogens
- PMID: 26856438
- PMCID: PMC7166946
- DOI: 10.1002/jmv.24492
Comparing Luminex NxTAG-Respiratory Pathogen Panel and RespiFinder-22 for multiplex detection of respiratory pathogens
Abstract
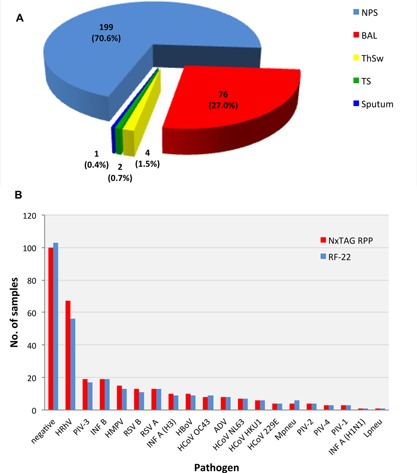
Respiratory tract infection (RTI) involves a variety of viruses and bacteria, which can be conveniently detected by multiplex nucleic acid amplification testing (NAT). To compare the novel Luminex-based NxTAG-Respiratory Pathogen Panel (NxTAG-RPP) with the routine multiplex-ligation-NAT based RespiFinder-22® (RF-22), 282 respiratory specimens including nasopharyngeal swabs (71%), broncho-alveolar lavage (27%), throat swabs, tracheal secretions, and sputum (2%) from 116 children and 155 adults were extracted using a Corbett CAS1200 (Qiagen), and analyzed in parallel by the routine RF-22 and NxTAG-RPP. Concordant results were obtained in 263 (93.3%) cases consisting of concordant positives in 167 (59.2%) and concordant negatives in 96 (34%). Results were discordant in 19 (6.7%) consisting of 15 positive:negative, and 4 negative:positive results by NxTAG-RPP versus RF-22, respectively. Co-infections were observed in 10.3% with NxTAG-RPP and in 5.9% with RF-22. Most additional viral pathogens identified by the NxTAG-RPP involved dual infections with rhinovirus and RSV. Discordant samples were mainly due to low genome signals of Ct less than 36, when retested by QNAT suggesting a higher sensitivity of the NxTAG-RPP, also when detecting multiple infections. Hands-on time after extraction for 24 and 96 samples was 0.25 and <0.5 hr for the NxTAG-RPP, and 2 and 4 hr for the RF-22, respectively. The median turn-around time was 6 hr (range 5-7 hr) for NxTAG-RPP and 12 hr (range 8-16 hr) for RF-22. The NxTAG-RPP showed comparable detection rates for most respiratory pathogens, while hands-on and turn-around time were considerably shorter. The clinical significance of detecting multiple viruses needs further clinical evaluation. J. Med. Virol. 88:1319-1324, 2016. © 2016 Wiley Periodicals, Inc.
Keywords: hands-on-time; multiplex PCR; nucleic acid testing; respiratory tract infection; respiratory tract infectious disease; turn-around-time.
© 2016 Wiley Periodicals, Inc.
Figures
References
-
- Grondahl B, Ankermann T, von Bismarck P, Rockahr S, Kowalzik F, Gehring S, Meyer C, Knuf M, Puppe W. 2014. The 2009 pandemic influenza A(H1N1) coincides with changes in the epidemiology of other viral pathogens causing acute respiratory tract infections in children. Infection 42:303–308. - PMC - PubMed
-
- Hirsch HH, Martino R, Ward KN, Boeckh M, Einsele H, Ljungman P. 2013. Fourth European conference on infections in leukaemia (ECIL‐4): Guidelines for diagnosis and treatment of human respiratory syncytial virus, parainfluenza virus, metapneumovirus, rhinovirus, and coronavirus. Clin Infect Dis 56:258–266. - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
