

Derivation and Multicenter Validation of the Drug Resistance in Pneumonia Clinical Prediction Score
- PMID: 26856838
- PMCID: PMC4862530
- DOI: 10.1128/AAC.03071-15
Derivation and Multicenter Validation of the Drug Resistance in Pneumonia Clinical Prediction Score
Abstract
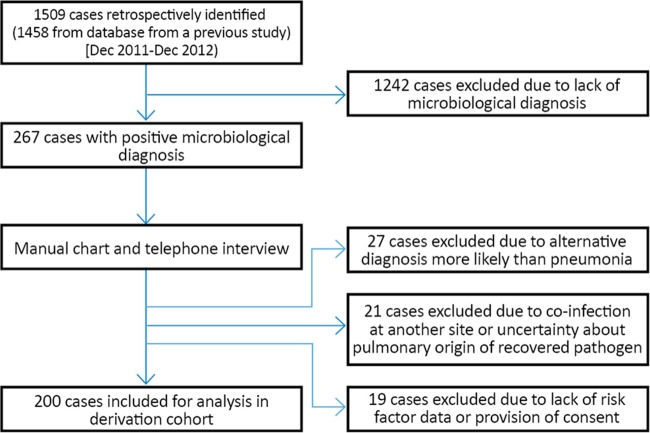
The health care-associated pneumonia (HCAP) criteria have a limited ability to predict pneumonia caused by drug-resistant bacteria and favor the overutilization of broad-spectrum antibiotics. We aimed to derive and validate a clinical prediction score with an improved ability to predict the risk of pneumonia due to drug-resistant pathogens compared to that of HCAP criteria. A derivation cohort of 200 microbiologically confirmed pneumonia cases in 2011 and 2012 was identified retrospectively. Risk factors for pneumonia due to drug-resistant pathogens were evaluated by logistic regression, and a novel prediction score (the drug resistance in pneumonia [DRIP] score) was derived. The score was then validated in a prospective, observational cohort of 200 microbiologically confirmed cases of pneumonia at four U.S. centers in 2013 and 2014. The DRIP score (area under the receiver operator curve [AUROC], 0.88 [95% confidence interval {CI}, 0.82 to 0.93]) performed significantly better (P = 0.02) than the HCAP criteria (AUROC, 0.72 [95% CI, 0.64 to 0.79]). At a threshold of ≥4 points, the DRIP score demonstrated a sensitivity of 0.82 (95% CI, 0.67 to 0.88), a specificity of 0.81 (95% CI, 0.73 to 0.87), a positive predictive value (PPV) of 0.68 (95% CI, 0.56 to 0.78), and a negative predictive value (NPV) of 0.90 (95% CI, 0.81 to 0.93). By comparison, the performance of HCAP criteria was less favorable: sensitivity was 0.79 (95% CI, 0.67 to 0.88), specificity was 0.65 (95% CI, 0.56 to 0.73), PPV was 0.53 (95% CI, 0.42 to 0.63), and NPV was 0.86 (95% CI, 0.77 to 0.92). The overall accuracy of the HCAP criteria was 69.5% (95% CI, 62.5 to 75.7%), whereas that of the DRIP score was 81.5% (95% CI, 74.2 to 85.6%) (P = 0.005). Unnecessary extended-spectrum antibiotics were recommended 46% less frequently by applying the DRIP score (25/200, 12.5%) than by use of HCAP criteria (47/200, 23.5%) (P = 0.004), without increasing the rate at which inadequate treatment recommendations were made. The DRIP score was more predictive of the risk of pneumonia due to drug-resistant pathogens than HCAP criteria and may have the potential to decrease antibiotic overutilization in patients with pneumonia. Validation in larger cohorts of patients with pneumonia due to all causes is necessary.
Copyright © 2016, American Society for Microbiology. All Rights Reserved.
Figures


Comment in
-
Application of the DRIP Score at a Veterans Affairs Hospital.Antimicrob Agents Chemother. 2018 Feb 23;62(3):e02277-17. doi: 10.1128/AAC.02277-17. Print 2018 Mar. Antimicrob Agents Chemother. 2018. PMID: 29475891 Free PMC article. No abstract available.
-
Reply to Babbel et al., "Application of the DRIP Score at a Veterans Affairs Hospital".Antimicrob Agents Chemother. 2018 Feb 23;62(3):e02337-17. doi: 10.1128/AAC.02337-17. Print 2018 Mar. Antimicrob Agents Chemother. 2018. PMID: 29475893 Free PMC article. No abstract available.
Similar articles
-
Validation of a scoring tool to predict drug-resistant pathogens in hospitalised pneumonia patients.Int J Tuberc Lung Dis. 2013 May;17(5):704-9. doi: 10.5588/ijtld.12.0723. Int J Tuberc Lung Dis. 2013. PMID: 23575340
-
Development and validation of a clinical risk score for predicting drug-resistant bacterial pneumonia in older Chinese patients.Respirology. 2014 May;19(4):549-55. doi: 10.1111/resp.12267. Epub 2014 Mar 24. Respirology. 2014. PMID: 24661357
-
Predicting risk of drug-resistant organisms in pneumonia: moving beyond the HCAP model.Respir Med. 2015 Jan;109(1):1-10. doi: 10.1016/j.rmed.2014.10.017. Epub 2014 Nov 13. Respir Med. 2015. PMID: 25468412 Review.
-
Risk factors for drug-resistant pathogens in community-acquired and healthcare-associated pneumonia.Am J Respir Crit Care Med. 2013 Oct 15;188(8):985-95. doi: 10.1164/rccm.201301-0079OC. Am J Respir Crit Care Med. 2013. PMID: 23855620
-
Empiric antibiotic selection and risk prediction of drug-resistant pathogens in community-onset pneumonia.Curr Opin Infect Dis. 2016 Apr;29(2):167-77. doi: 10.1097/QCO.0000000000000254. Curr Opin Infect Dis. 2016. PMID: 26886179 Review.
Cited by
-
Derivation and Validation of a Clinical Prediction Score to Identify the Isolation of Pseudomonas in Pneumonia.Microbiol Spectr. 2022 Jun 29;10(3):e0042422. doi: 10.1128/spectrum.00424-22. Epub 2022 May 23. Microbiol Spectr. 2022. PMID: 35604182 Free PMC article.
-
PES Pathogens in Severe Community-Acquired Pneumonia.Microorganisms. 2019 Feb 12;7(2):49. doi: 10.3390/microorganisms7020049. Microorganisms. 2019. PMID: 30759805 Free PMC article. Review.
-
Calculated parenteral initial treatment of bacterial infections: Economic aspects of antibiotic treatment.GMS Infect Dis. 2020 Mar 26;8:Doc03. doi: 10.3205/id000047. eCollection 2020. GMS Infect Dis. 2020. PMID: 32373428 Free PMC article.
-
Deploying an Electronic Clinical Decision Support Tool for Diagnosis and Treatment of Pneumonia Into Rural and Critical Access Hospitals: Utilization, Effect on Processes of Care, and Clinician Satisfaction.J Rural Health. 2022 Jan;38(1):262-269. doi: 10.1111/jrh.12543. Epub 2020 Nov 26. J Rural Health. 2022. PMID: 33244803 Free PMC article.
-
Simulated Adoption of 2019 Community-Acquired Pneumonia Guidelines Across 114 Veterans Affairs Medical Centers: Estimated Impact on Culturing and Antibiotic Selection in Hospitalized Patients.Clin Infect Dis. 2021 Jan 29;72(Suppl 1):S59-S67. doi: 10.1093/cid/ciaa1604. Clin Infect Dis. 2021. PMID: 33512530 Free PMC article.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
