

Impact of an Emergency Department Observation Unit Management Algorithm for Atrial Fibrillation
- PMID: 26857070
- PMCID: PMC4802469
- DOI: 10.1161/JAHA.115.002984
Impact of an Emergency Department Observation Unit Management Algorithm for Atrial Fibrillation
Abstract
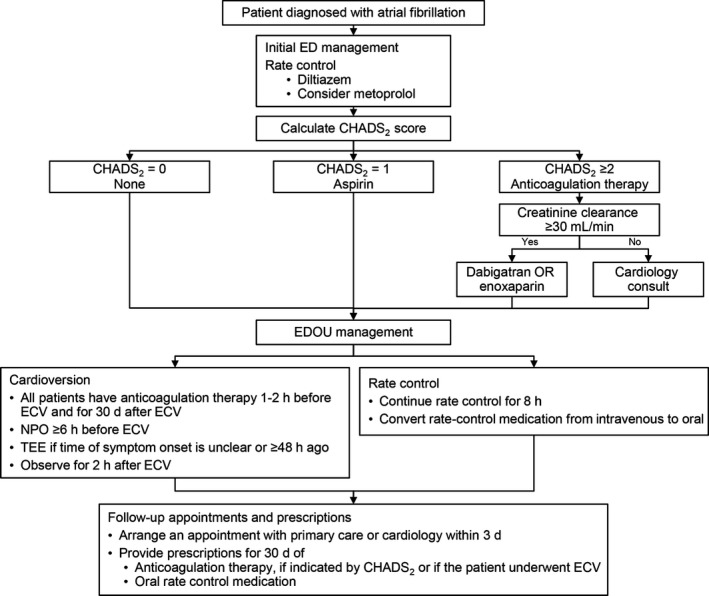
Background: Atrial fibrillation (AF) is a common, growing, and costly medical condition. We aimed to evaluate the impact of a management algorithm for symptomatic AF that used an emergency department observation unit on hospital admission rates and patient outcomes.
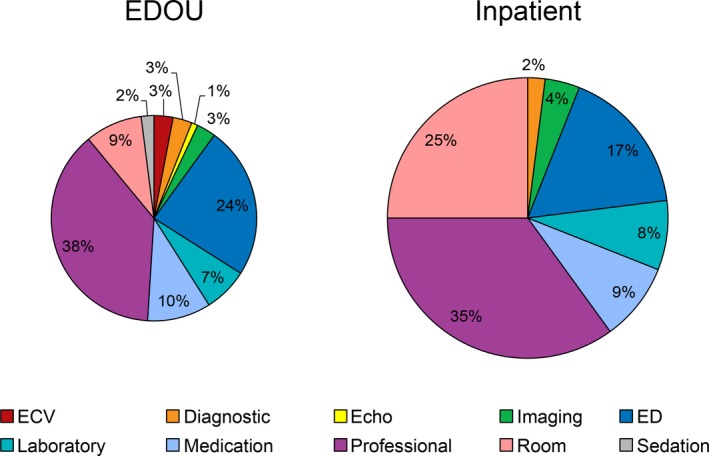
Methods and results: This retrospective cohort study compared 563 patients who presented consecutively in the year after implementation of the algorithm, from July 2013 through June 2014 (intervention group), with 627 patients in a historical cohort (preintervention group) who presented consecutively from July 2011 through June 2012. All patients who consented to have their records used for chart review were included if they had a primary final emergency department diagnosis of AF. We observed no significant differences in age, sex, vital signs, body mass index, or CHADS2 (congestive heart failure, hypertension, age, diabetes mellitus, and prior stroke or transient ischemic attack) score between the preintervention and intervention groups. The rate of inpatient admission was significantly lower in the intervention group (from 45% to 36%; P<0.001). The groups were not significantly different with regard to rates of return emergency department visits (19% versus 17%; P=0.48), hospitalization (18% versus 16%; P=0.22), or adverse events (2% versus 2%; P=0.95) within 30 days. Emergency department observation unit admissions were 40% (P<0.001) less costly than inpatient hospital admissions of ≤1 day's duration.
Conclusions: Implementation of an emergency department observation unit AF algorithm was associated with significantly decreased hospital admissions without increasing the rates of return emergency department visits, hospitalization, or adverse events within 30 days.
Keywords: anticoagulants; arrhythmia; fibrillation.
© 2016 The Authors. Published on behalf of the American Heart Association, Inc., by Wiley Blackwell.
Figures
References
-
- Fuster V, Rydén LE, Cannom DS, Crijns HJ, Curtis AB, Ellenbogen KA, Halperin JL, Kay GN, Le Huezey J‐Y, Lowe JE, Olsson SB, Prystowsky EN, Tamargo JL, Wann LS. 2011 ACCF/AHA/HRS focused updates incorporated into the ACC/AHA/ESC 2006 guidelines for the management of patients with atrial fibrillation: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines developed in partnership with the European Society of Cardiology and in collaboration with the European Heart Rhythm Association and the Heart Rhythm Society. J Am Coll Cardiol. 2011;57:e101–e198. - PubMed
-
- Atzema CL, Austin PC, Miller E, Chong AS, Yun L, Dorian P. A population‐based description of atrial fibrillation in the emergency department, 2002 to 2010. Ann Emerg Med. 2013;62:570–577.e577. - PubMed
-
- McDonald AJ, Pelletier AJ, Ellinor PT, Camargo CA Jr. Increasing US emergency department visit rates and subsequent hospital admissions for atrial fibrillation from 1993 to 2004. Ann Emerg Med. 2008;51:58–65. - PubMed
-
- Kim MH, Johnston SS, Chu BC, Dalal MR, Schulman KL. Estimation of total incremental health care costs in patients with atrial fibrillation in the United States. Circ Cardiovasc Qual Outcomes. 2011;4:313–320. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
