

Effectiveness of Remote Patient Monitoring After Discharge of Hospitalized Patients With Heart Failure: The Better Effectiveness After Transition -- Heart Failure (BEAT-HF) Randomized Clinical Trial
- PMID: 26857383
- PMCID: PMC4827701
- DOI: 10.1001/jamainternmed.2015.7712
Effectiveness of Remote Patient Monitoring After Discharge of Hospitalized Patients With Heart Failure: The Better Effectiveness After Transition -- Heart Failure (BEAT-HF) Randomized Clinical Trial
Erratum in
-
Error in Text and Table.JAMA Intern Med. 2016 Apr;176(4):568. doi: 10.1001/jamainternmed.2016.0624. JAMA Intern Med. 2016. PMID: 26974880 Free PMC article. No abstract available.
-
Updated Supplement.JAMA Intern Med. 2016 Jun 1;176(6):871. doi: 10.1001/jamainternmed.2016.1684. JAMA Intern Med. 2016. PMID: 27089116 No abstract available.
Abstract
Importance: It remains unclear whether telemonitoring approaches provide benefits for patients with heart failure (HF) after hospitalization.
Objective: To evaluate the effectiveness of a care transition intervention using remote patient monitoring in reducing 180-day all-cause readmissions among a broad population of older adults hospitalized with HF.
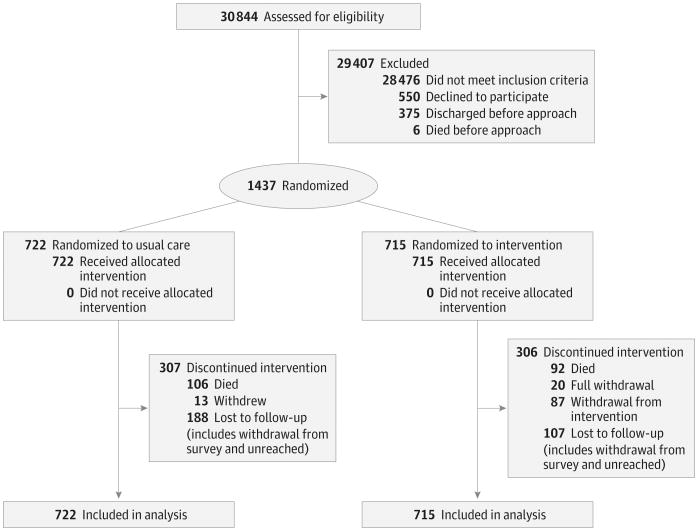
Design, setting, and participants: We randomized 1437 patients hospitalized for HF between October 12, 2011, and September 30, 2013, to the intervention arm (715 patients) or to the usual care arm (722 patients) of the Better Effectiveness After Transition-Heart Failure (BEAT-HF) study and observed them for 180 days. The dates of our study analysis were March 30, 2014, to October 1, 2015. The setting was 6 academic medical centers in California. Participants were hospitalized individuals 50 years or older who received active treatment for decompensated HF.
Interventions: The intervention combined health coaching telephone calls and telemonitoring. Telemonitoring used electronic equipment that collected daily information about blood pressure, heart rate, symptoms, and weight. Centralized registered nurses conducted telemonitoring reviews, protocolized actions, and telephone calls.
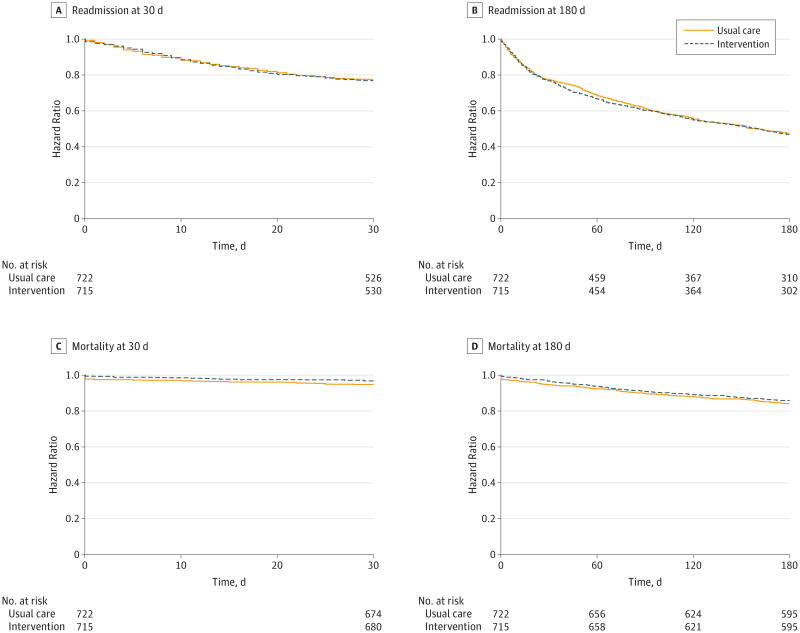
Main outcomes and measures: The primary outcome was readmission for any cause within 180 days after discharge. Secondary outcomes were all-cause readmission within 30 days, all-cause mortality at 30 and 180 days, and quality of life at 30 and 180 days.
Results: Among 1437 participants, the median age was 73 years. Overall, 46.2% (664 of 1437) were female, and 22.0% (316 of 1437) were African American. The intervention and usual care groups did not differ significantly in readmissions for any cause 180 days after discharge, which occurred in 50.8% (363 of 715) and 49.2% (355 of 722) of patients, respectively (adjusted hazard ratio, 1.03; 95% CI, 0.88-1.20; P = .74). In secondary analyses, there were no significant differences in 30-day readmission or 180-day mortality, but there was a significant difference in 180-day quality of life between the intervention and usual care groups. No adverse events were reported.
Conclusions and relevance: Among patients hospitalized for HF, combined health coaching telephone calls and telemonitoring did not reduce 180-day readmissions.
Trial registration: clinicaltrials.gov Identifier: NCT01360203.
Conflict of interest statement
Figures
Comment in
-
New Approaches to Reduce Readmissions in Patients With Heart Failure.JAMA Intern Med. 2016 Mar;176(3):318-20. doi: 10.1001/jamainternmed.2015.7993. JAMA Intern Med. 2016. PMID: 26857025 No abstract available.
-
Transition care with telemonitoring did not reduce readmission after hospitalization for heart failure.Ann Intern Med. 2016 May 17;164(10):JC59. doi: 10.7326/ACPJC-2016-164-10-059. Ann Intern Med. 2016. PMID: 27182925 No abstract available.
-
Telemedicine in Heart Failure-Ineffective or Just Ill Used?JAMA Intern Med. 2016 Jul 1;176(7):1034-5. doi: 10.1001/jamainternmed.2016.2854. JAMA Intern Med. 2016. PMID: 27379483 No abstract available.
-
Telemedicine in Heart Failure-Ineffective or Just Ill Used?JAMA Intern Med. 2016 Jul 1;176(7):1035. doi: 10.1001/jamainternmed.2016.2857. JAMA Intern Med. 2016. PMID: 27379484 No abstract available.
-
Telemedicine in Heart Failure-Ineffective or Just Ill Used?-Reply.JAMA Intern Med. 2016 Jul 1;176(7):1035-6. doi: 10.1001/jamainternmed.2016.2860. JAMA Intern Med. 2016. PMID: 27379485 No abstract available.
References
-
- Gheorghiade M, Vaduganathan M, Fonarow GC, Bonow RO. Rehospitalization for heart failure: problems and perspectives. J Am Coll Cardiol. 2013;61(4):391–403. - PubMed
-
- Thom T, Haase N, Rosamond W, et al. American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Heart disease and stroke statistics: 2006 update: a report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee [published corrections appear in Circulation. 2006;113(14):e696 and 2006;114(23):e630] Circulation. 2006;113(6):e85–e151. doi: 10.1161/CIRCULATIONAHA.105.171600. - DOI - PubMed
-
- Jencks SF, Williams MV, Coleman EA. Rehospitalizations among patients in the Medicare fee-for-service program [published correction appears in N Engl J Med. 2011;364(16):1582] N Engl J Med. 2009;360(14):1418–1428. - PubMed
-
- Centers for Medicare & Medicaid Services. [Accessed September 28, 2015];Hospital Compare. https://www.medicare.gov/hospitalcompare/search.html.
-
- Krumholz HM, Merrill AR, Schone EM, et al. Patterns of hospital performance in acute myocardial infarction and heart failure 30-day mortality and readmission. Circ Cardiovasc Qual Outcomes. 2009;2(5):407–413. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
