

Malperfusion syndromes in aortic dissections
- PMID: 26858183
- PMCID: PMC4876056
- DOI: 10.1177/1358863X15625371
Malperfusion syndromes in aortic dissections
Abstract
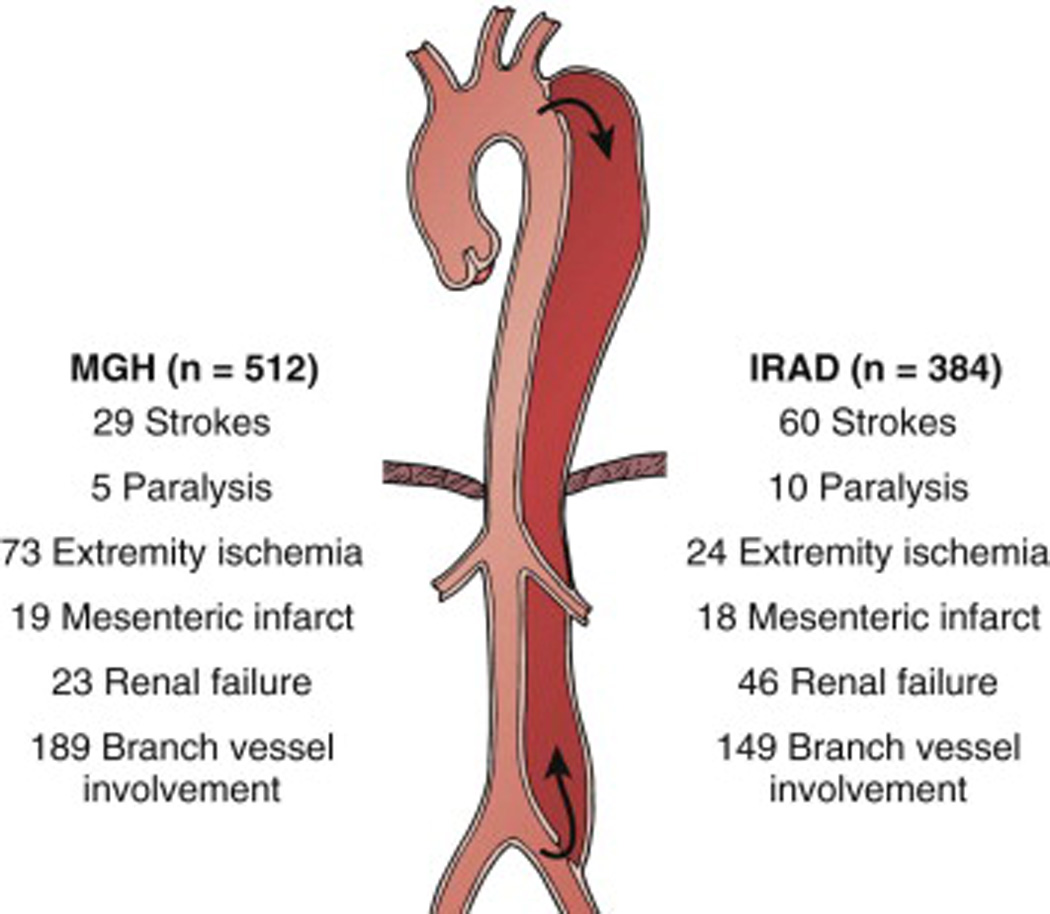
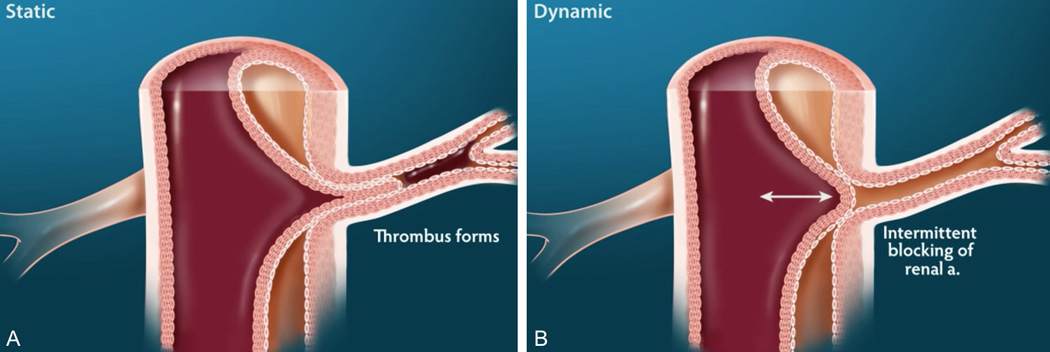
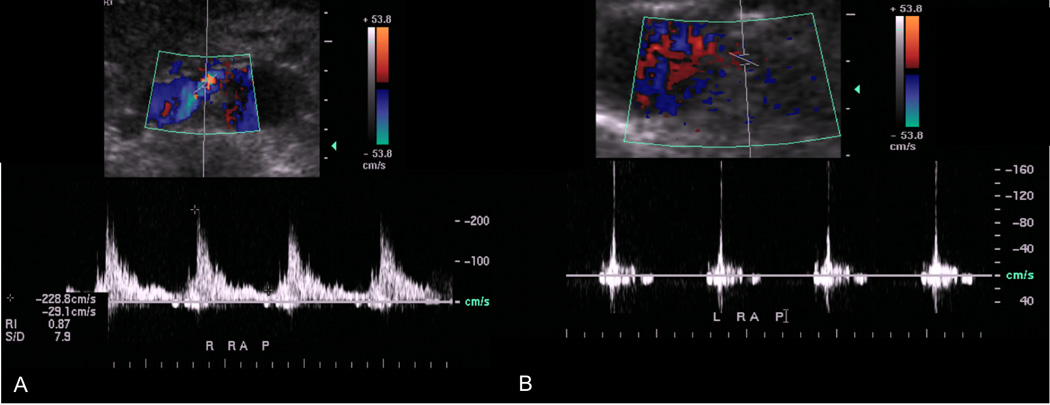
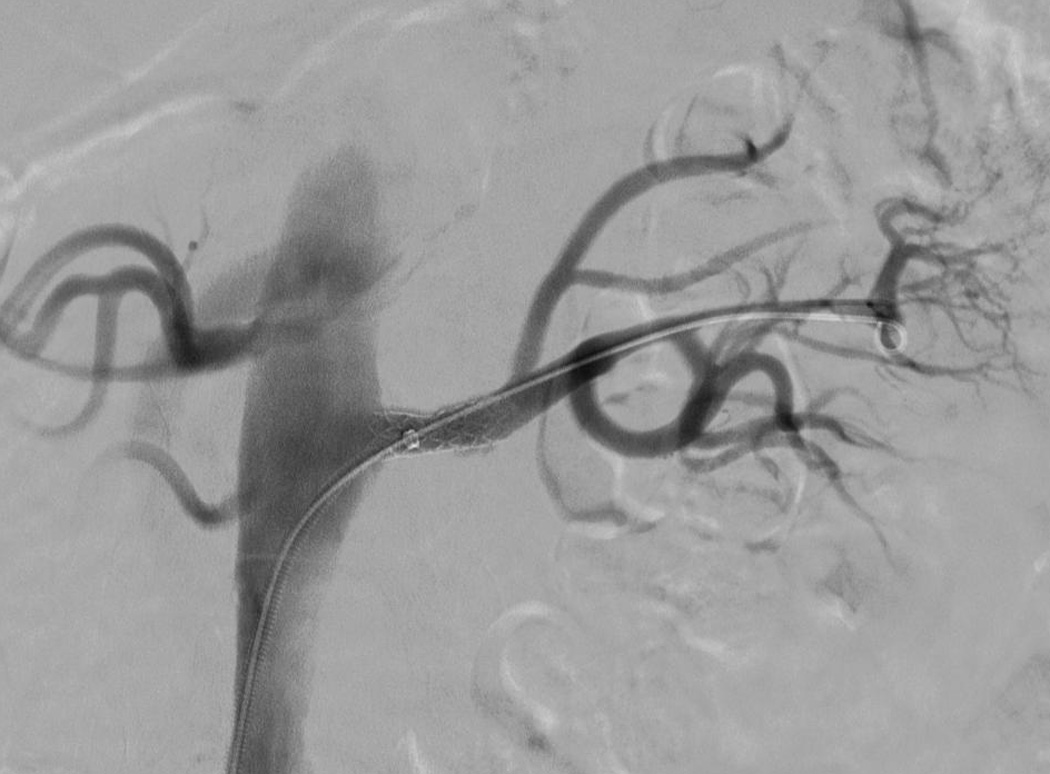
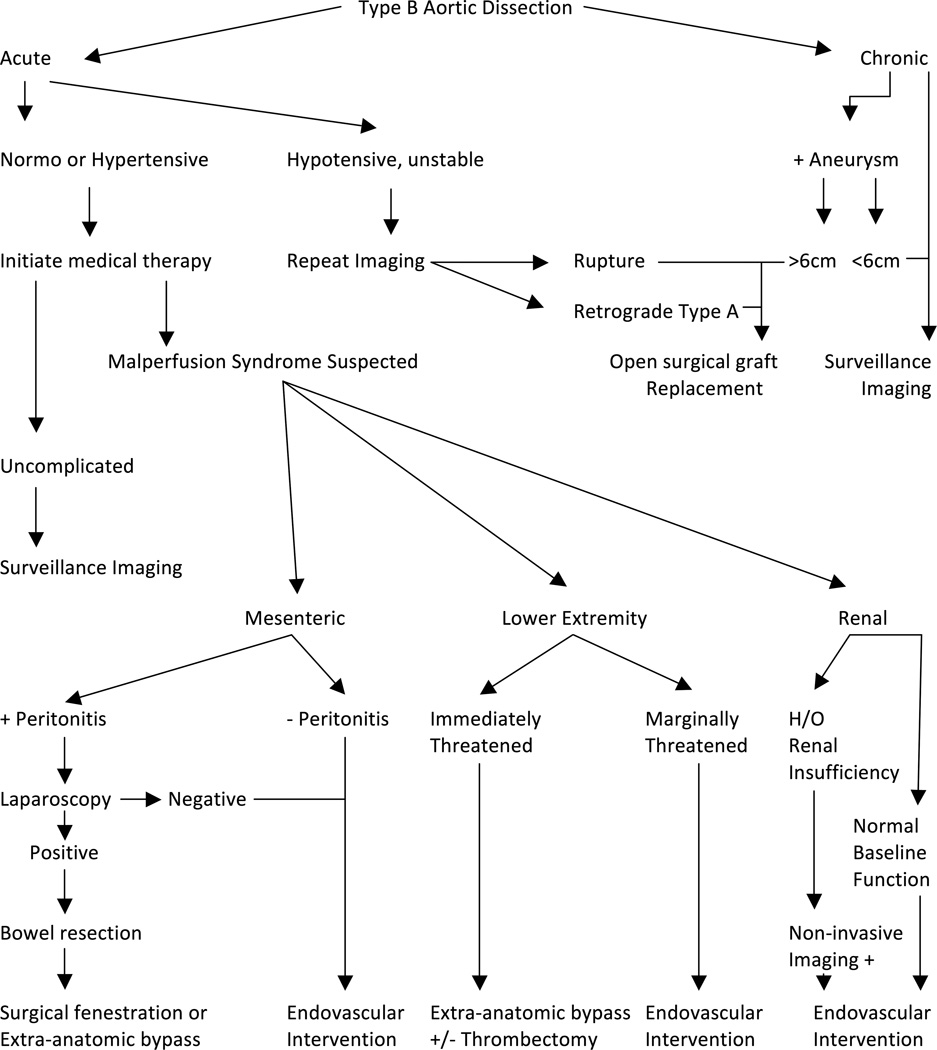
Aortic dissection remains a challenging clinical scenario, especially when complicated by peripheral malperfusion. Improvements in medical imaging have furthered understanding of the pathophysiology of malperfusion events in association with aortic dissection, including the elucidation of different mechanisms of branch vessel obstruction. Despite these advances, malperfusion syndrome remains a deadly entity with significant mortality. This review presents the latest knowledge regarding the pathogenesis of aortic dissection complicated by malperfusion syndrome, and discusses the diagnostic and therapeutic guidelines for management of this vicious entity.
Keywords: aortic diseases; minimally invasive; practice guidelines; stents; surgical procedures.
© The Author(s) 2016.
Figures

Similar articles
-
Experience of the Zenith Dissection Endovascular System in the emergency setting of malperfusion in acute type B dissections.J Vasc Surg. 2014 Mar;59(3):645-50. doi: 10.1016/j.jvs.2013.09.004. Epub 2013 Nov 16. J Vasc Surg. 2014. PMID: 24246535
-
Simultaneous fenestration with stent implantation for acute limb ischemia due to type B acute aortic dissection complicated with both static and dynamic obstructions.Ann Thorac Cardiovasc Surg. 2012;18(2):158-61. doi: 10.5761/atcs.cr.11.01712. Epub 2011 Oct 28. Ann Thorac Cardiovasc Surg. 2012. PMID: 22033242
-
Malperfusion, Malperfusion Syndrome, and Mesenteric Ischemia in Aortic Dissection.Semin Thorac Cardiovasc Surg. 2025 Summer;37(2):132-135. doi: 10.1053/j.semtcvs.2024.11.005. Epub 2024 Dec 8. Semin Thorac Cardiovasc Surg. 2025. PMID: 39657896 Review.
-
Endovascular fenestration in aortic dissection with acute malperfusion syndrome: immediate and late follow-up.J Thorac Cardiovasc Surg. 2011 Jul;142(1):66-72. doi: 10.1016/j.jtcvs.2010.07.081. J Thorac Cardiovasc Surg. 2011. PMID: 21683839
-
Visceral Malperfusion in Aortic Dissection: The Michigan Experience.Semin Thorac Cardiovasc Surg. 2017 Summer;29(2):173-178. doi: 10.1053/j.semtcvs.2016.10.002. Epub 2016 Oct 14. Semin Thorac Cardiovasc Surg. 2017. PMID: 28823323 Review.
Cited by
-
Delayed Surgical Management of Acute Type A Aortic Dissection in a Patient with Recent COVID-19 Infection and Post-COVID-19 Bronchopneumonia-Case Report and Review of Literature.Medicina (Kaunas). 2022 Sep 27;58(10):1357. doi: 10.3390/medicina58101357. Medicina (Kaunas). 2022. PMID: 36295518 Free PMC article. Review.
-
Beyond Atherosclerosis and Fibromuscular Dysplasia: Rare Causes of Renovascular Hypertension.Hypertension. 2021 Sep;78(4):898-911. doi: 10.1161/HYPERTENSIONAHA.121.17004. Epub 2021 Aug 30. Hypertension. 2021. PMID: 34455817 Free PMC article. Review.
-
The role of delayed aortic surgery in type A aortic dissection and mesenteric ischemia: a systematic review and meta-analysis.J Cardiothorac Surg. 2023 Aug 18;18(1):247. doi: 10.1186/s13019-023-02341-y. J Cardiothorac Surg. 2023. PMID: 37596605 Free PMC article.
-
Risk factors of acute kidney injury in patients with Stanford type B aortic dissection involving the renal artery who underwent thoracic endovascular aortic repair.Ren Fail. 2021 Dec;43(1):1130-1136. doi: 10.1080/0886022X.2021.1949349. Ren Fail. 2021. PMID: 35048774 Free PMC article.
-
Outcomes and risk management in type B aortic dissection patients with acute kidney injury: a concise review.Ren Fail. 2021 Dec;43(1):585-596. doi: 10.1080/0886022X.2021.1905664. Ren Fail. 2021. PMID: 33784934 Free PMC article. Review.
References
-
- Fann JI, Smith JA, Miller DC, et al. Surgical management of aortic dissection during a 30-year period. Circulation. 1995 Nov 1;92(9 Suppl):II113–II121. - PubMed
-
- DeBakey ME, McCollum CH, Crawford ES, et al. Dissection and dissecting aneurysms of the aorta: twenty-year follow-up of five hundred twenty-seven patients treated surgically. Surgery. 1982 Dec;92(6):1118–1134. - PubMed
-
- Cambria RP, Brewster DC, Gertler J, et al. Vascular complications associated with spontaneous aortic dissection. J Vasc Surg. 1988 Feb;7(2):199–209. - PubMed
-
- O'Gara PT, DeSanctis RW. Acute aortic dissection and its variants. Toward a common diagnostic and therapeutic approach. Circulation. 1995 Sep 15;92(6):1376–1378. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
