

Longitudinal Assessment of Neurocognitive Outcomes in Survivors of Childhood Acute Lymphoblastic Leukemia Treated on a Contemporary Chemotherapy Protocol
- PMID: 26858334
- PMCID: PMC4872325
- DOI: 10.1200/JCO.2015.64.3205
Longitudinal Assessment of Neurocognitive Outcomes in Survivors of Childhood Acute Lymphoblastic Leukemia Treated on a Contemporary Chemotherapy Protocol
Abstract
Purpose: Survivors of childhood acute lymphoblastic leukemia (ALL) treated with CNS-directed chemotherapy are at risk for neurocognitive deficits. Prospective longitudinal studies are needed to clarify the neurodevelopmental trajectory in this vulnerable population.
Methods: Patients enrolled in the St. Jude Total Therapy Study XV, which omitted prophylactic cranial radiation therapy in all patients, completed comprehensive neuropsychological assessments at induction (n = 142), end of maintenance (n = 243), and 2 years after completion of therapy (n = 211). We report on longitudinal change in neurocognitive function and predictors of neurocognitive outcomes 2 years after completing therapy.
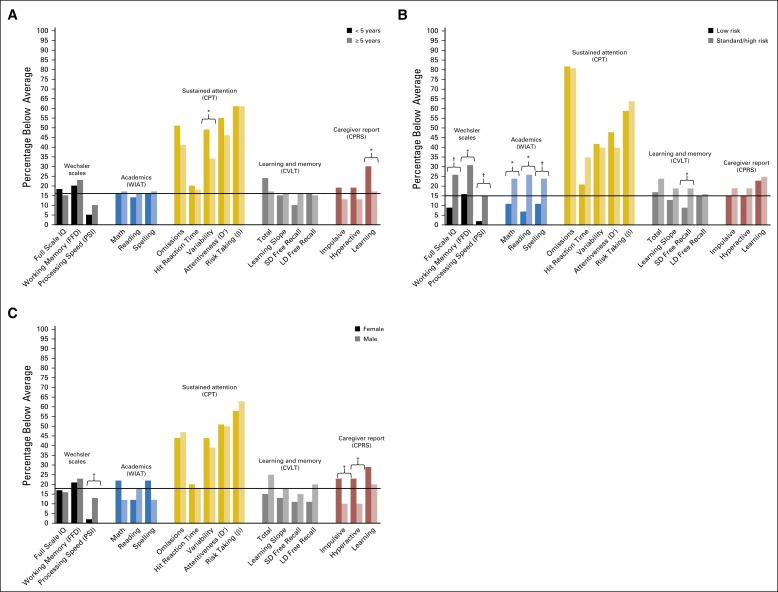
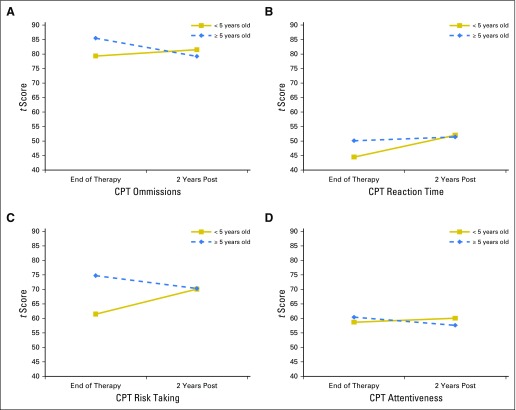
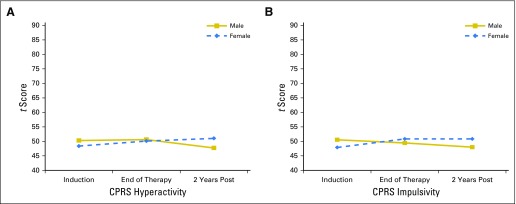
Results: Neurocognitive function was largely age appropriate 2 years after completing therapy; however, the overall group demonstrated significant attention deficits and a significantly greater frequency of learning problems as compared with national normative data (all P ≤ .005). Higher-intensity CNS-directed chemotherapy conferred elevated risk for difficulties in attention, processing speed, and academics (all P ≤ .01). The rate and direction of change in performance and caregiver-reported attention difficulties differed significantly by age at diagnosis and sex. End-of-therapy attention problems predicted lower academic scores 2 years later, with small to moderate effect sizes (│r│= 0.17 to 0.25, all P ≤ .05).
Conclusion: Two years after chemotherapy-only treatment, neurocognitive function is largely age appropriate. Nonetheless, survivors remain at elevated risk for attention problems that impact real-world functioning. Attention problems at the end of therapy predicted decreased academics 2 years later, suggesting an amplified functional impact of discrete neurocognitive difficulties. Age at diagnosis and patient sex may alter neurocognitive development in survivors of childhood ALL treated with chemotherapy-only protocols.
© 2016 by American Society of Clinical Oncology.
Conflict of interest statement
Authors’ disclosures of potential conflicts of interest are found in the article online at
Figures
References
-
- Kaatsch P. Epidemiology of childhood cancer. Cancer Treat Rev. 2010;36:277–285. - PubMed
-
- Jankovic M, Brouwers P, Valsecchi MG, et al. International Study Group on Psychosocial Aspects of Childhood Cancer Association of 1800 cGy cranial irradiation with intellectual function in children with acute lymphoblastic leukaemia. ISPACC. Lancet. 1994;344:224–227. - PubMed
-
- Langer T, Martus P, Ottensmeier H, et al. CNS late-effects after ALL therapy in childhood. Part III: neuropsychological performance in long-term survivors of childhood ALL: Impairments of concentration, attention, and memory. Med Pediatr Oncol. 2002;38:320–328. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
