

Protocol for Bone Augmentation with Simultaneous Early Implant Placement: A Retrospective Multicenter Clinical Study
- PMID: 26858757
- PMCID: PMC4672140
- DOI: 10.1155/2015/589135
Protocol for Bone Augmentation with Simultaneous Early Implant Placement: A Retrospective Multicenter Clinical Study
Abstract
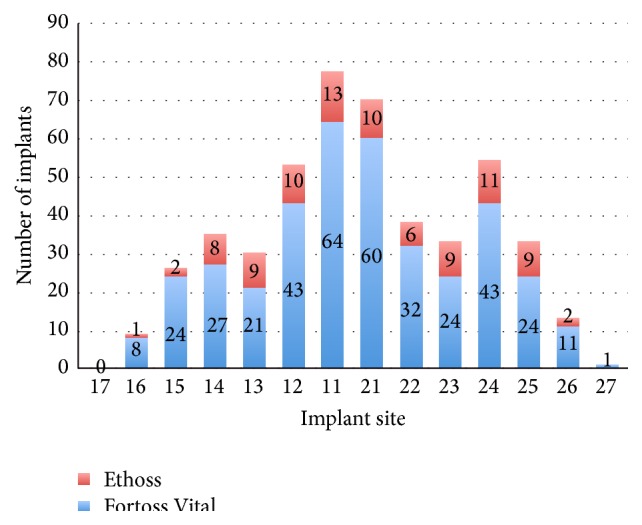
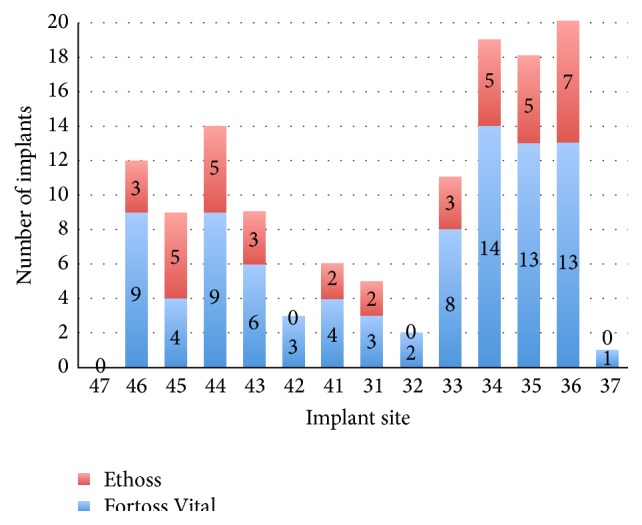
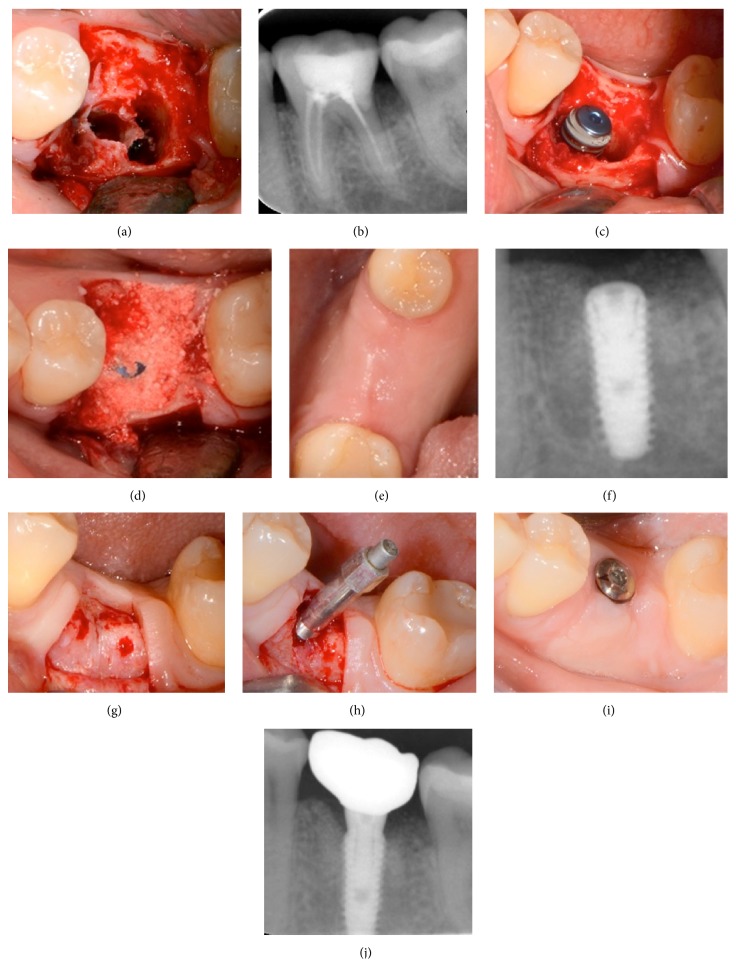
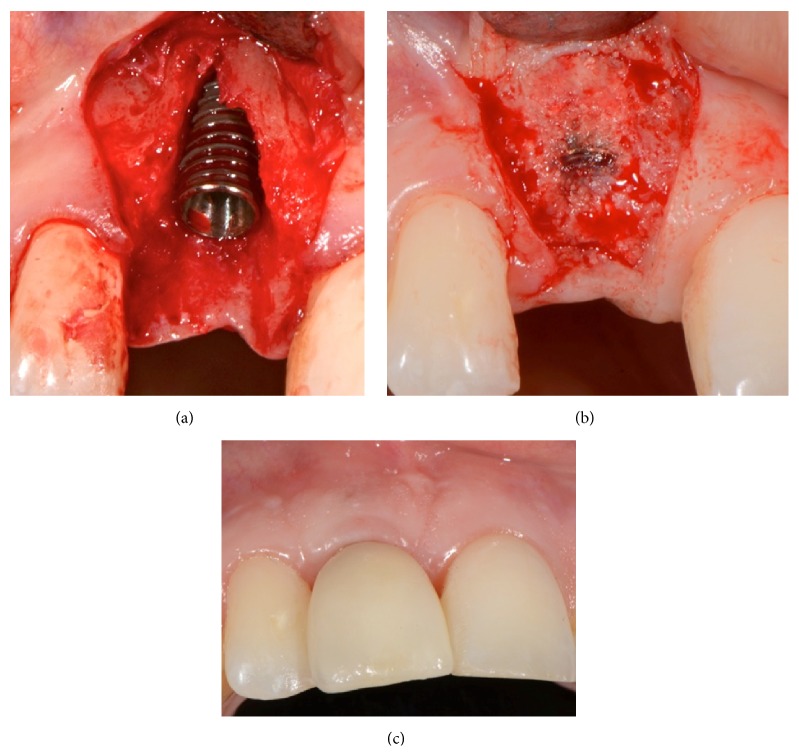
Purpose. To present a novel protocol for alveolar bone regeneration in parallel to early implant placement. Methods. 497 patients in need of extraction and early implant placement with simultaneous bone augmentation were treated in a period of 10 years. In all patients the same specific method was followed and grafting was performed utilizing in situ hardening fully resorbable alloplastic grafting materials consisting of β-tricalcium phosphate and calcium sulfate. The protocol involved atraumatic extraction, implant placement after 4 weeks with simultaneous bone augmentation, and loading of the implant 12 weeks after placement and grafting. Follow-up periods ranged from 6 months to 10 years (mean of 4 years). Results. A total of 601 postextraction sites were rehabilitated in 497 patients utilizing the novel protocol. Three implants failed before loading and three implants failed one year after loading, leaving an overall survival rate of 99.0%. Conclusions. This standardized protocol allows successful long-term functional results regarding alveolar bone regeneration and implant rehabilitation. The concept of placing the implant 4 weeks after extraction, augmenting the bone around the implant utilizing fully resorbable, biomechanically stable, alloplastic materials, and loading the implant at 12 weeks seems to offer advantages when compared with traditional treatment modalities.
Figures

Similar articles
-
Clinical evaluation alveolar ridge preservation with a beta-tricalcium phosphate socket graft.Compend Contin Educ Dent. 2009 Nov-Dec;30(9):588-90, 592, 594 passim; quiz 604, 606. Compend Contin Educ Dent. 2009. PMID: 19998726
-
Immediate loading of tapered implants placed in postextraction sockets: retrospective analysis of the 5-year clinical outcome.Clin Implant Dent Relat Res. 2012 Aug;14(4):565-74. doi: 10.1111/j.1708-8208.2010.00297.x. Epub 2010 Jul 17. Clin Implant Dent Relat Res. 2012. PMID: 20662861
-
Localized lateral alveolar ridge augmentation with block bone grafts: simultaneous versus delayed implant placement: a clinical and radiographic retrospective study.Int J Oral Maxillofac Implants. 2013 May-Jun;28(3):846-53. doi: 10.11607/jomi.2964. Int J Oral Maxillofac Implants. 2013. PMID: 23748318
-
Immediate or early placement of implants following tooth extraction: review of biologic basis, clinical procedures, and outcomes.Int J Oral Maxillofac Implants. 2004;19 Suppl:12-25. Int J Oral Maxillofac Implants. 2004. PMID: 15635942 Review.
-
Simultaneous implant placement and bone grafting with particulate mineralized allograft in sites with buccal wall defects, a three-year follow-up and review of literature.J Craniomaxillofac Surg. 2014 Jul;42(5):552-9. doi: 10.1016/j.jcms.2013.07.026. Epub 2013 Aug 22. J Craniomaxillofac Surg. 2014. PMID: 24529349 Review.
Cited by
-
New Insights in Hydrogels for Periodontal Regeneration.J Funct Biomater. 2023 Nov 11;14(11):545. doi: 10.3390/jfb14110545. J Funct Biomater. 2023. PMID: 37998114 Free PMC article. Review.
-
Bone Healing in Rabbit Calvaria Defects Using a Synthetic Bone Substitute: A Histological and Micro-CT Comparative Study.Materials (Basel). 2018 Oct 17;11(10):2004. doi: 10.3390/ma11102004. Materials (Basel). 2018. PMID: 30336544 Free PMC article.
-
Sinus Augmentation for Implant Placement Utilizing a Novel Synthetic Graft Material with Delayed Immediate Socket Grafting: A 2-Year Case Study.J Clin Med. 2023 Mar 24;12(7):2485. doi: 10.3390/jcm12072485. J Clin Med. 2023. PMID: 37048568 Free PMC article.
-
Evaluation of an In Situ Hardening β-Tricalcium Phosphate Graft Material for Alveolar Ridge Preservation. A Histomorphometric Animal Study in Pigs.Dent J (Basel). 2018 Jul 2;6(3):27. doi: 10.3390/dj6030027. Dent J (Basel). 2018. PMID: 30004400 Free PMC article.
-
Bone Grafts and Substitutes in Dentistry: A Review of Current Trends and Developments.Molecules. 2021 May 18;26(10):3007. doi: 10.3390/molecules26103007. Molecules. 2021. PMID: 34070157 Free PMC article. Review.
References
-
- Chen S. T., Wilson T. G., Jr., Hämmerle C. H. F. Immediate or early placement of implants following tooth extraction: review of biologic basis, clinical procedures, and outcomes. The International Journal of Oral & Maxillofacial Implants. 2004;19(19):12–25. - PubMed
-
- Esposito M., Grusovin M. G., Polyzos I. P., Felice P., Worthington H. V. Timing of implant placement after tooth extraction: immediate, immediate-delayed or delayed implants? A Cochrane systematic review. European Journal of Oral Implantology. 2010;3(3):189–205. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
