

Posterior Reversible Encephalopathy Syndrome Resolving Within 48 Hours in a Normotensive Patient Who Underwent Thoracic Spine Surgery
- PMID: 26858804
- PMCID: PMC4737042
- DOI: 10.14740/jocmr2472w
Posterior Reversible Encephalopathy Syndrome Resolving Within 48 Hours in a Normotensive Patient Who Underwent Thoracic Spine Surgery
Abstract
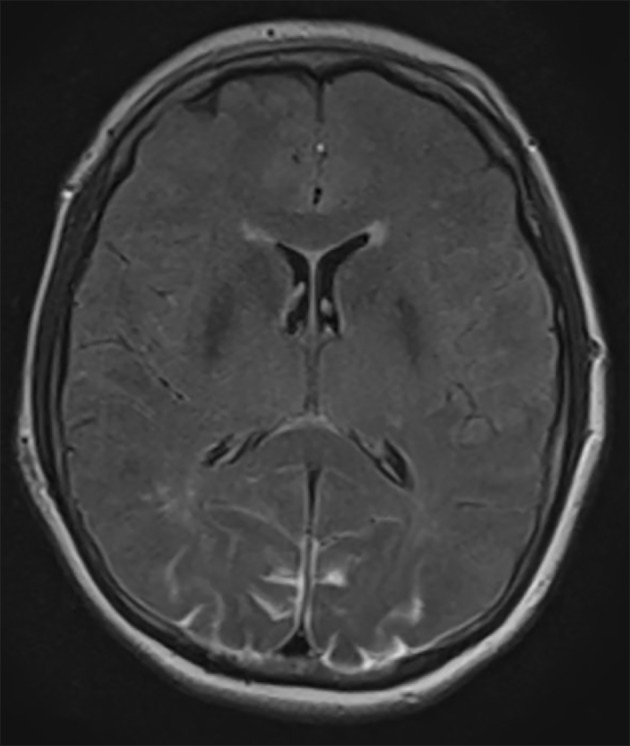
Posterior reversible encephalopathy syndrome (PRES) usually manifests with severe headaches, seizures, and visual disturbances due to uncontrollable hypertension. A patient (age in the early 60s) with a history of renal cell cancer presented with lower-extremity weakness and paresthesias. Magnetic resonance imaging (MRI) of the thoracic spine revealed a T8 vertebral body metastatic lesion with cord compression at that level. The patient underwent preoperative embolization of the tumor followed by posterior resection and placement of percutaneous pedicle screws and rods. Postoperatively, the patient experienced decreased visual acuity bilaterally. Abnormal MRI findings consisted of T2 hyperintense lesions and fluid-attenuated inversion recovery changes in both occipital lobes, consistent with the unique brain imaging pattern associated with PRES. The patient's blood pressure was normal and stable from the first day of hospitalization. The patient was kept on high-dose steroid therapy, which was started intraoperatively, and improved within 48 hours after symptom onset.
Keywords: Cortical blindness; Posterior reversible encephalopathy syndrome; Prone surgery.
Figures

References
-
- Stambough JL, Dolan D, Werner R, Godfrey E. Ophthalmologic complications associated with prone positioning in spine surgery. J Am Acad Orthop Surg. 2007;15(3):156–165. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources