

One-Year Mortality in Older Patients with Cancer: Development and External Validation of an MNA-Based Prognostic Score
- PMID: 26859298
- PMCID: PMC4747505
- DOI: 10.1371/journal.pone.0148523
One-Year Mortality in Older Patients with Cancer: Development and External Validation of an MNA-Based Prognostic Score
Abstract
Purpose: The MNA (Mini Nutritional Assessment) is known as a prognosis factor in older population. We analyzed the prognostic value for one-year mortality of MNA items in older patients with cancer treated with chemotherapy as the basis of a simplified prognostic score.
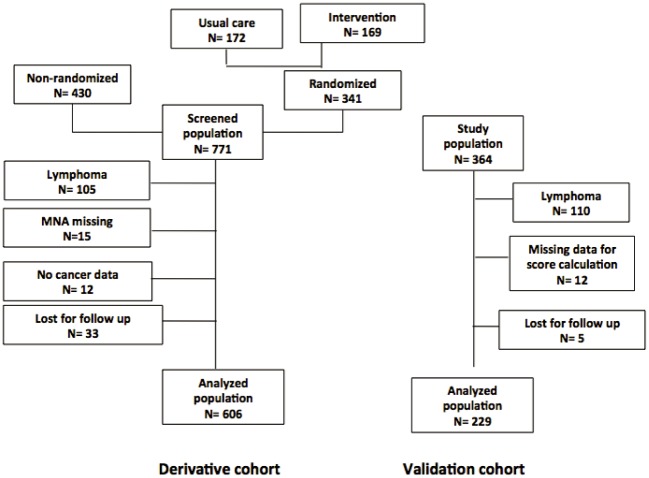
Methods: The prospective derivation cohort included 606 patients older than 70 years with an indication of chemotherapy for cancers. The endpoint to predict was one-year mortality. The 18 items of the Full MNA, age, gender, weight loss, cancer origin, TNM, performance status and lymphocyte count were considered to construct the prognostic model. MNA items were analyzed with a backward step-by-step multivariate logistic regression and other items were added in a forward step-by-step regression. External validation was performed on an independent cohort of 229 patients.
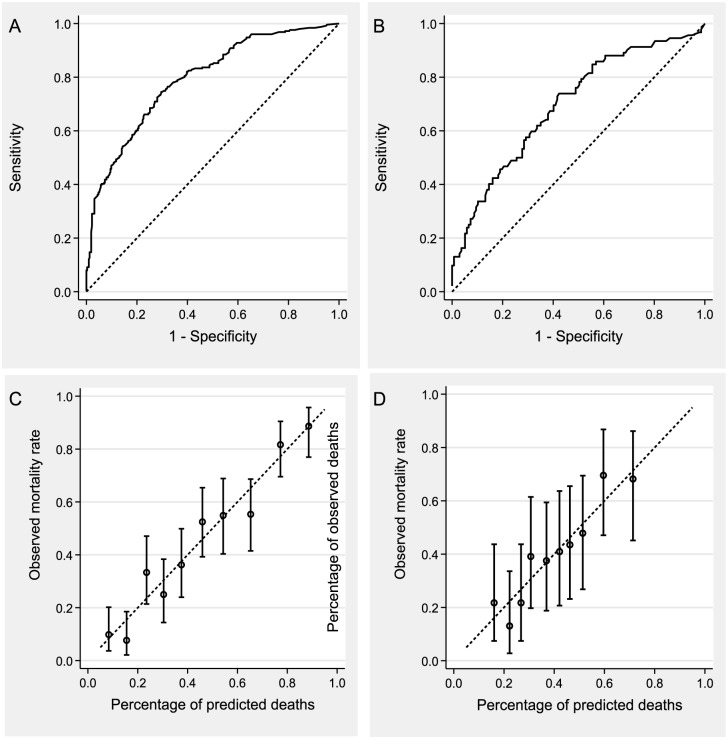
Results: At one year 266 deaths had occurred. Decreased dietary intake (p = 0.0002), decreased protein-rich food intake (p = 0.025), 3 or more prescribed drugs (p = 0.023), calf circumference <31 cm (p = 0.0002), tumor origin (p<0.0001), metastatic status (p = 0.0007) and lymphocyte count <1500/mm3 (0.029) were found to be associated with 1-year mortality in the final model and were used to construct a prognostic score. The area under curve (AUC) of the score was 0.793, which was higher than the Full MNA AUC (0.706). The AUC of the score in validation cohort (229 subjects, 137 deaths) was 0.698.
Conclusion: Key predictors of one-year mortality included cancer cachexia clinical features, comorbidities, the origin and the advanced status of the tumor. The prognostic value of this model combining a subset of MNA items and cancer related items was better than the full MNA, thus providing a simple score to predict 1-year mortality in older patients with an indication of chemotherapy.
Conflict of interest statement
Figures
References
-
- Extermann M, Aapro M, Bernabei R, Cohen HJ, Droz JP, Lichtman S, et al. Use of comprehensive geriatric assessment in older cancer patients: recommendations from the task force on CGA of the International Society of Geriatric Oncology (SIOG). Critical reviews in oncology/hematology. 2005;55(3):241–52. . - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
