

Pharmacodynamics and Pharmacokinetics Following Once-Daily and Twice-Daily Dosing of Tiotropium Respimat® in Asthma Using Standardized Sample-Contamination Avoidance
- PMID: 26859538
- PMCID: PMC5073218
- DOI: 10.1089/jamp.2015.1260
Pharmacodynamics and Pharmacokinetics Following Once-Daily and Twice-Daily Dosing of Tiotropium Respimat® in Asthma Using Standardized Sample-Contamination Avoidance
Abstract
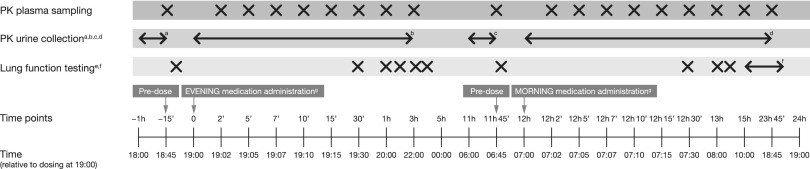
Background: This study was conducted to confirm the 24-hour bronchodilator efficacy and pharmacokinetic profile of once-daily tiotropium Respimat® 5 μg add-on to inhaled corticosteroids (ICS) in adults with symptomatic asthma. It used a trial protocol designed to minimize the risk of pharmacokinetic sample contamination resulting from improper sampling procedure, sample handling, or device handling during priming and subsequent inhalation procedure.
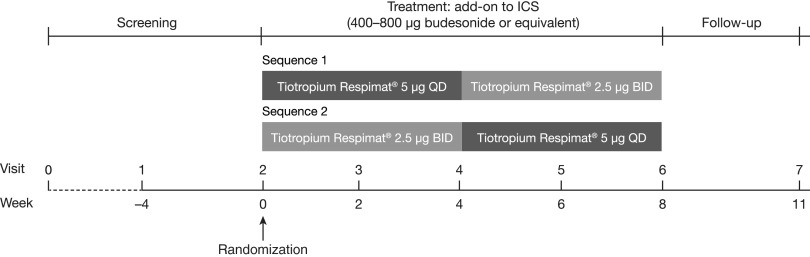
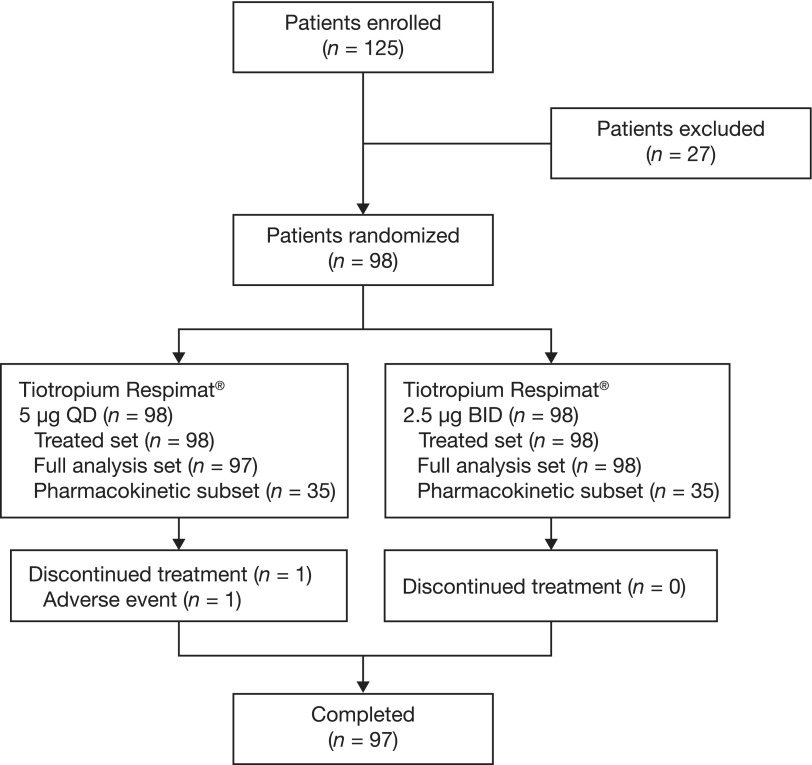
Methods: A Phase II, randomized, double-blind, two-way crossover study (NCT01696071) comparing two daily dosing regimens of tiotropium for 4 weeks, once-daily 5 μg (evening dosing) or twice-daily 2.5 μg (morning and evening dosing), as add-on to maintenance therapy with ICS (400-800 μg budesonide or equivalent) as controller medication. There was no washout between treatment periods.
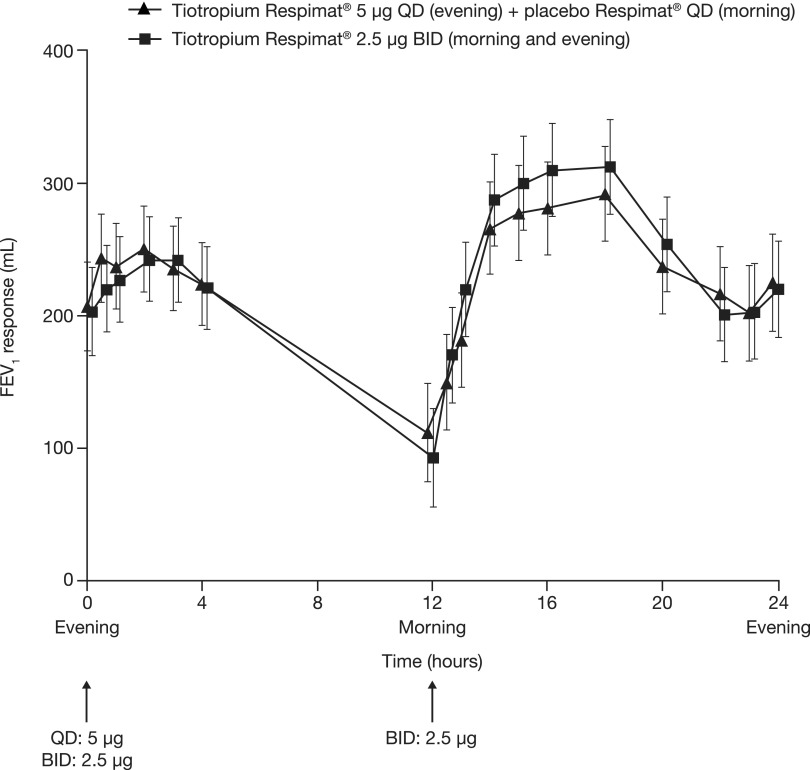
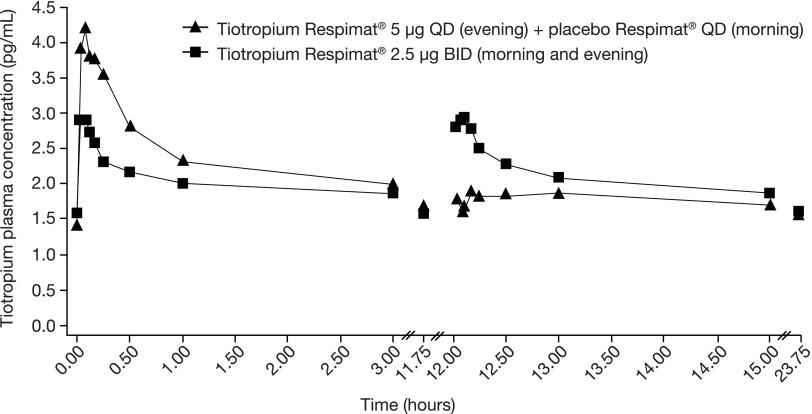
Results: An increase in the area under the curve of the 24-hour forced expiratory volume in 1 second profile from study baseline was observed following once-daily tiotropium 5 μg (217 mL) and twice-daily 2.5 μg (219 mL), with no difference between the two regimens (-2 mL [95% confidence interval: -38, 34]). In a subset of the study population, total tiotropium exposure, expressed as area under the plasma concentration versus time curve over 24 hours, was comparable between dosing regimens. Unexpected tiotropium plasma levels were observed in two patients, possibly because of contamination.
Conclusions: The observed bronchodilator efficacy over 24 hours was similar with once-daily tiotropium 5 μg and twice-daily 2.5 μg as add-on to ICS therapy, supporting the suitability of once-daily dosing to provide sustained improvements in lung function in adults with symptomatic asthma.
Keywords: Respimat®; asthma; blood-sampling contamination; pharmacodynamics; pharmacokinetics; tiotropium.
Conflict of interest statement
Author Disclosure Statement K-MB is employed by insaf Respiratory Research Institute GmbH and has received compensation from various pharmaceutical companies for organizing or participating in advisory board and scientific meetings, and for the design, performance, or participation in single- or multicenter clinical trials. RD has received personal fees from Boehringer Ingelheim, Novartis, GlaxoSmithKline, and Almirall, outside the submitted work. DD has received consulting fees, lecturing fees, and payment from Boehringer Ingelheim for the development of educational activities. A-MK is employed by Pulmonary Research Institute at LungClinic Grosshansdorf, which has been compensated for the conduct of the study, and received compensation for scientific meetings or lectures from various pharmaceutical companies, including Boehringer Ingelheim. AS, RS, and PMZ are employees of, and PC is a former employee of, Boehringer Ingelheim.
Figures
References
-
- Bateman ED, Boushey HA, Bousquet J, Busse WW, Clark TJH, Pauwels RA, Pedersen SE, and for the GOAL Investigators Group: Can guideline-defined asthma control be achieved? The Gaining Optimal Asthma ControL study. Am J Respir Crit Care Med. 2004;170:836–844 - PubMed
-
- Demoly P, Paggiaro P, Plaza V, Bolge SC, Kannan H, Sohier B, and Adamek L: Prevalence of asthma control among adults in France, Germany, Italy, Spain and the UK. Eur Respir Rev. 2009;18:105–112 - PubMed
-
- Ivanova JI, Bergman R, Birnbaum HG, Colice GL, Silverman RA, and McLaurin K: Effect of asthma exacerbations on health care costs among asthmatic patients with moderate and severe persistent asthma. J Allergy Clin Immunol. 2012;129:1229–1235 - PubMed
-
- Braman SS: The global burden of asthma. Chest. 2006;130:4S–12S - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources