

Outcome of EMR as an alternative to surgery in patients with complex colon polyps
- PMID: 26859866
- PMCID: PMC4949087
- DOI: 10.1016/j.gie.2016.01.067
Outcome of EMR as an alternative to surgery in patients with complex colon polyps
Abstract
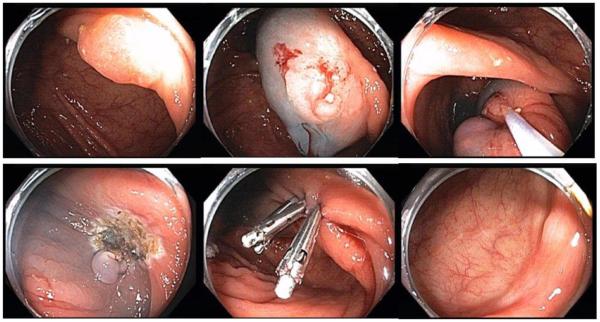
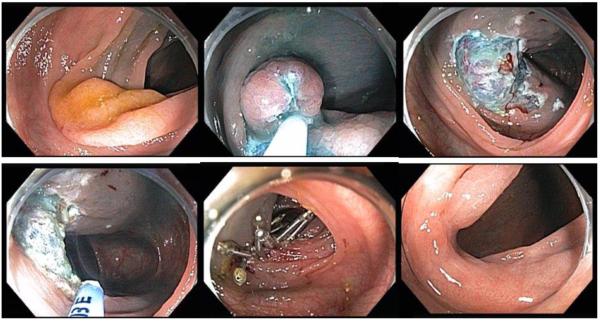
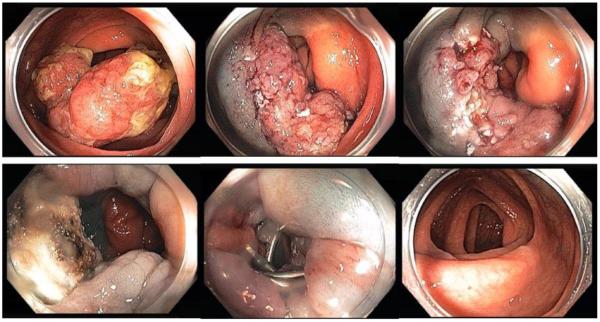
Background and aims: Patients with complex colon polyps were traditionally referred for surgery to avoid adverse events associated with endoscopic resection. Recent advances in endoscopic imaging as well as endoscopic hemostasis and clip closure allow for the use of EMR as an alternative to surgery for such lesions. To determine the outcome of treatment of complex colon polyps with EMR as an alternative to surgery, we conducted a retrospective observational study.
Methods: Two hundred three patients with complex colon polyps were referred to an EMR center as an alternative to surgery. Patients underwent a protocol-driven EMR. The primary endpoint was the complete resection rate. Secondary endpoints were safety, residual adenoma rate, and incidence of missed synchronous polyps.
Results: EMR was performed in 155 patients and was deferred in 48 patients who were referred to surgery. EMR specimens revealed benign polyps in 149 and cancer in 6 patients. EMR adverse events occurred in 7 patients, requiring hospitalization in 5 of them. None of the patients died as a result of their adverse events. Surveillance colonoscopy at 4 to 6 months after resection of a benign lesion in 137 patients revealed residual adenoma at the scar site in 6 patients and additional synchronous precancerous lesions in 117 patients that were not removed by the referring endoscopist. None underwent surgery for failure of EMR. The overall precancerous lesion burden was 2.83 per patient, the adenoma burden was 2.13 per patient, and the serrated polyp burden was .69 per patient.
Conclusions: EMR can be used instead of surgery for complex colon polyps in 75% of patients with few adverse events and few residual adenomas at resection sites. In addition, careful repeat examination of the entire colon for synchronous lesions overlooked by the referring endoscopist is required for most patients. (
Clinical trial registration number: NCT01827241.).
Copyright © 2016 American Society for Gastrointestinal Endoscopy. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
EMR should be the first-line treatment for large laterally spreading colorectal lesions.Gastrointest Endosc. 2016 Aug;84(2):326-8. doi: 10.1016/j.gie.2016.03.1508. Gastrointest Endosc. 2016. PMID: 27425801 No abstract available.
Similar articles
-
Outcomes of EMR of defiant colorectal lesions directed to an endoscopy referral center.Gastrointest Endosc. 2012 Aug;76(2):255-63. doi: 10.1016/j.gie.2012.02.060. Epub 2012 May 31. Gastrointest Endosc. 2012. PMID: 22657404
-
Cold Versus Hot Snare Endoscopic Resection of Large Nonpedunculated Colorectal Polyps: Randomized Controlled German CHRONICLE Trial.Gastroenterology. 2024 Sep;167(4):764-777. doi: 10.1053/j.gastro.2024.05.013. Epub 2024 May 23. Gastroenterology. 2024. PMID: 38795735 Clinical Trial.
-
En bloc endoscopic mucosal resection is equally effective for sessile serrated polyps and conventional adenomas.Surg Endosc. 2018 Apr;32(4):1871-1878. doi: 10.1007/s00464-017-5876-3. Epub 2017 Sep 22. Surg Endosc. 2018. PMID: 28940106
-
Colorectal endoscopic mucosal resection (EMR).Best Pract Res Clin Gastroenterol. 2017 Aug;31(4):455-471. doi: 10.1016/j.bpg.2017.05.006. Epub 2017 Jun 13. Best Pract Res Clin Gastroenterol. 2017. PMID: 28842056 Review.
-
Cold snare endoscopic resection of nonpedunculated colorectal polyps larger than 10 mm: a systematic review and pooled-analysis.Gastrointest Endosc. 2019 May;89(5):929-936.e3. doi: 10.1016/j.gie.2018.12.022. Epub 2019 Jan 9. Gastrointest Endosc. 2019. PMID: 30639542
Cited by
-
Underwater endoscopic mucosal resection is associated with fewer recurrences and earlier curative resections compared to conventional endoscopic mucosal resection for large colorectal polyps.Surg Endosc. 2017 Oct;31(10):4174-4183. doi: 10.1007/s00464-017-5474-4. Epub 2017 Mar 24. Surg Endosc. 2017. PMID: 28342125
-
Endoscopic submucosal dissection in the treatment of patients with early colorectal carcinoma and precancerous lesions.J Gastrointest Oncol. 2020 Oct;11(5):911-917. doi: 10.21037/jgo-20-393. J Gastrointest Oncol. 2020. PMID: 33209487 Free PMC article.
-
Technical success, resection status, and procedural complication rate of colonoscopic full-wall resection: a pooled analysis from 7 hospitals of different care levels.Surg Endosc. 2021 Jul;35(7):3339-3353. doi: 10.1007/s00464-020-07772-5. Epub 2020 Jul 9. Surg Endosc. 2021. PMID: 32648038 Free PMC article.
-
Post-EMR for colorectal polyps, thermal ablation of defects reduces adenoma recurrence: A meta-analysis.Endosc Int Open. 2022 Oct 17;10(10):E1399-E1405. doi: 10.1055/a-1922-7646. eCollection 2022 Oct. Endosc Int Open. 2022. PMID: 36262518 Free PMC article. Review.
-
Impact of observational training on endoscopic mucosal resection outcomes and competency for large colorectal polyps: single endoscopist experience.Endosc Int Open. 2020 Mar;8(3):E346-E353. doi: 10.1055/a-1107-2711. Epub 2020 Feb 21. Endosc Int Open. 2020. PMID: 32140557 Free PMC article.
References
-
- Rex DK, Schoenfeld PS, Cohen J, et al. Quality indicators for colonoscopy. Gastrointest Endosc. 2015;81:31–53. - PubMed
-
- Sanchez-Yague A, Kaltenbach T, Raju G, et al. Advanced endoscopic resection of colorectal lesions. Gastroenterol Clin North Am. 2013;42:459–77. - PubMed
-
- Rutter MD, Nickerson C, Rees CJ, et al. Risk factors for adverse events related to polypectomy in the English Bowel Cancer Screening Programme. Endoscopy. 2014;46:90–7. - PubMed
-
- Belderbos TD, Leenders M, Moons LM, et al. Local recurrence after endoscopic mucosal resection of nonpedunculated colorectal lesions: systematic review and meta-analysis. Endoscopy. 2014;46:388–402. - PubMed
-
- Aziz Aadam A, Wani S, Kahi C, et al. Physician assessment and management of complex colon polyps: a multicenter video-based survey study. Am J Gastroenterol. 2014;109:1312–24. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
