

Baseline Characteristics and Prescription Patterns of Standard Drugs in Patients with Angiographically Determined Coronary Artery Disease and Renal Failure (CAD-REF Registry)
- PMID: 26859890
- PMCID: PMC4747471
- DOI: 10.1371/journal.pone.0148057
Baseline Characteristics and Prescription Patterns of Standard Drugs in Patients with Angiographically Determined Coronary Artery Disease and Renal Failure (CAD-REF Registry)
Abstract
Background: Chronic kidney disease (CKD) is strongly associated with coronary artery disease (CAD). We established a prospective observational nationwide multicenter registry to evaluate current treatment and outcomes in patients with both CKD and angiographically documented CAD.
Methods: In 32 cardiological centers 3,352 CAD patients with ≥50% stenosis in at least one coronary artery were enrolled and classified according to their estimated glomerular filtration rate and proteinuria into one of five stages of CKD or as a control group.
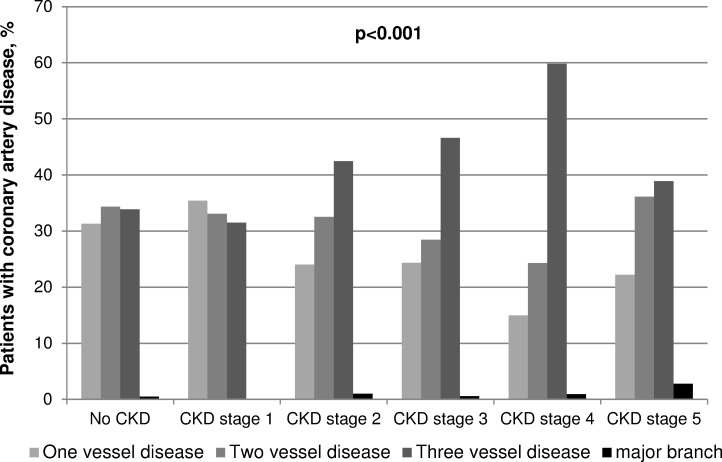
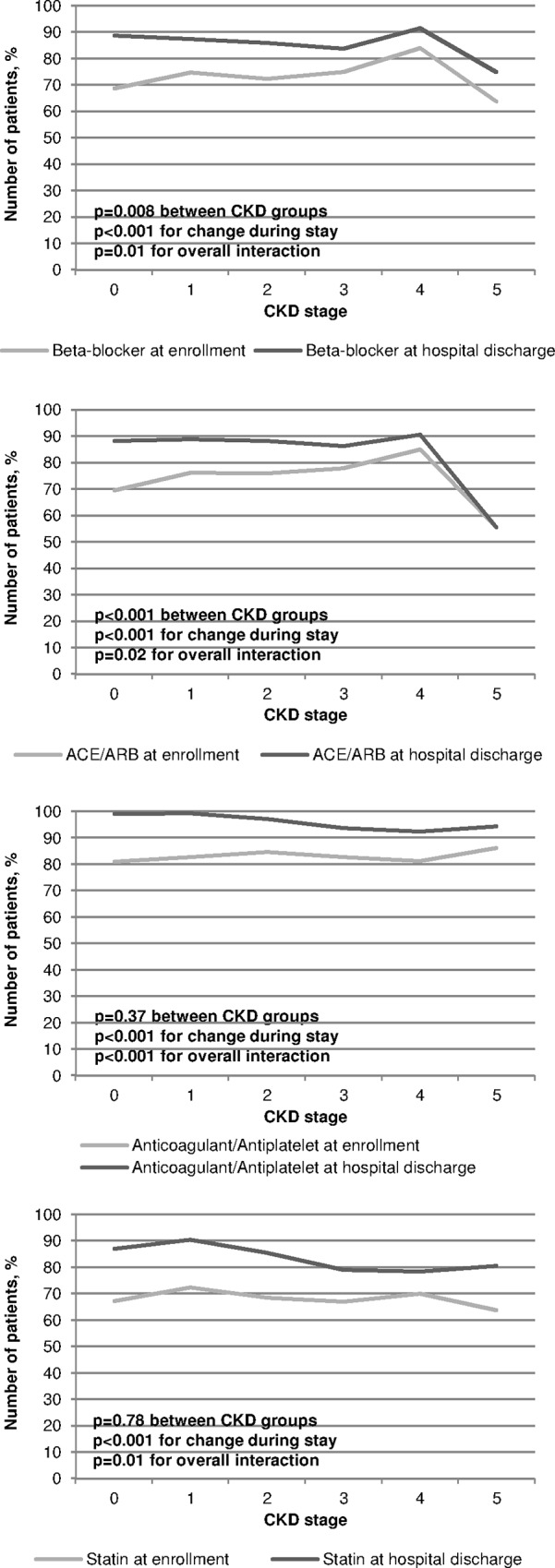
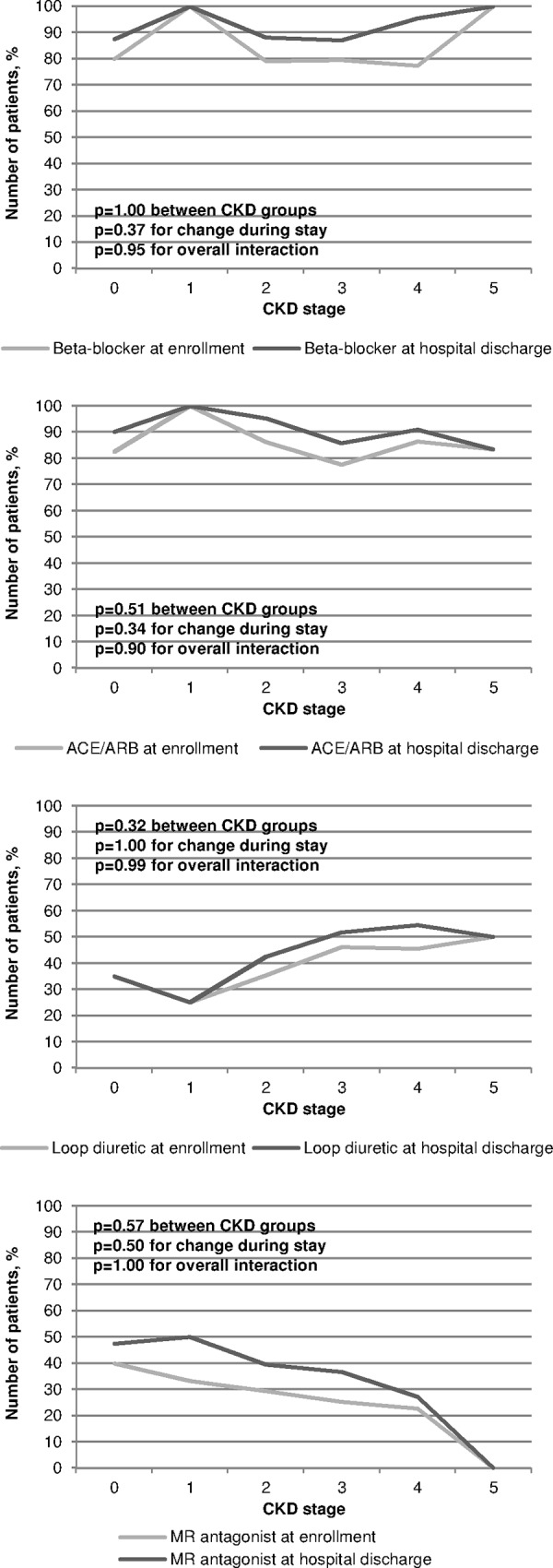
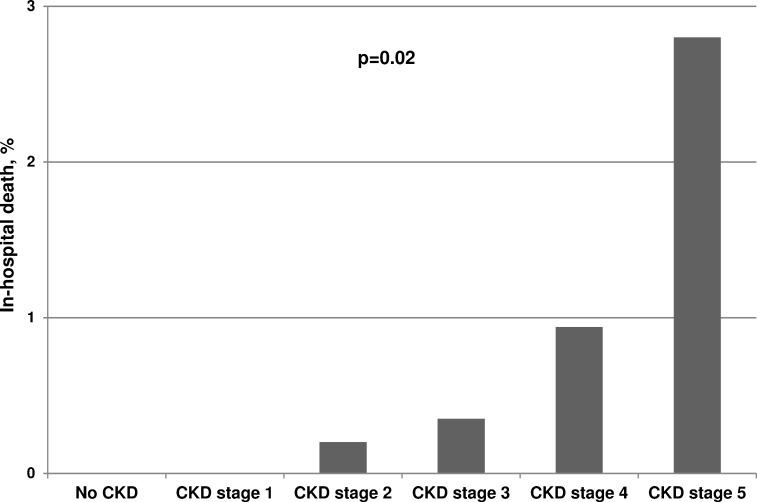
Results: 2,723 (81.2%) consecutively enrolled patients suffered from CKD. Compared to controls, CKD patients had a higher prevalence of diabetes, hypertension, peripheral artery diseases, heart failure, and valvular heart disease (each p<0.001). Myocardial infarctions (p = 0.02), coronary bypass grafting, valve replacements and pacemaker implantations had been recorded more frequently (each p<0.001). With advanced CKD, the number of diseased coronary vessels and the proportion of patients with reduced left ventricular ejection fraction (LVEF) increased significantly (both p<0.001). Percutaneous coronary interventions were performed less frequently (p<0.001) while coronary bypass grafting was recommended more often (p = 0.04) with advanced CKD. With regard to standard drugs in CAD treatment, prescriptions were higher in our registry than in previous reports, but beta-blockers (p = 0.008), and angiotensin-converting-enzyme inhibitors and/or angiotensin-receptor blockers (p<0.001) were given less often in higher CKD stages. In contrast, in the subgroup of patients with moderately to severely reduced LVEF the prescription rates did not differ between CKD stages. In-hospital mortality increased stepwise with each CKD stage (p = 0.02).
Conclusions: In line with other studies comprising CKD cohorts, patients' morbidity and in-hospital mortality increased with the degree of renal impairment. Although cardiologists' drug prescription rates in CAD-REF were higher than in previous studies, they were still lower especially in advanced CKD stages compared to cohorts treated by nephrologists.
Conflict of interest statement
Figures
References
-
- Levey AS, Atkins R, Coresh J, Cohen EP, Collins AJ, Eckardt KU, et al. Chronic kidney disease as a global public health problem: approaches and initiatives—a position statement from Kidney Disease Improving Global Outcomes. Kidney Int. 2007;72:247–259. - PubMed
-
- Sarnak MJ, Levey AS, Schoolwerth AC, Coresh J, Culleton B, Hamm LL, et al. Kidney disease as a risk factor for development of cardiovascular disease: a statement from the American Heart Association Councils on Kidney in Cardiovascular Disease, High Blood Pressure Research, Clinical Cardiology, and Epidemiology and Prevention. Circulation. 2003;108:2154–2169. - PubMed
-
- Go AS, Chertow GM, Fan D, McCulloch CE, Hsu CY. Chronic kidney disease and the risks of death, cardiovascular events, and hospitalization. N Engl J Med. 2004;351:1296–1305. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
