

Idiopathic Retroperitoneal Fibrosis
- PMID: 26860343
- PMCID: PMC4926988
- DOI: 10.1681/ASN.2015101110
Idiopathic Retroperitoneal Fibrosis
Abstract
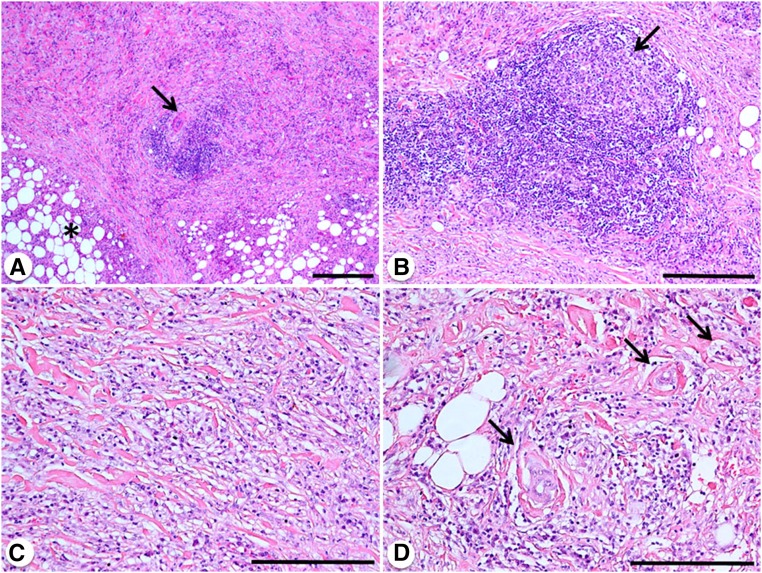
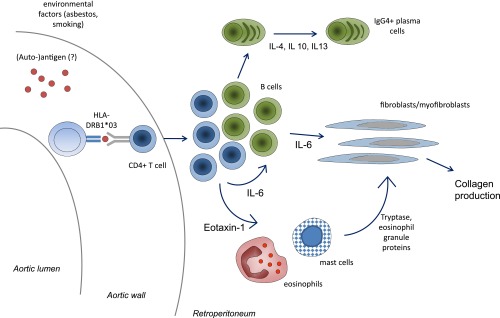
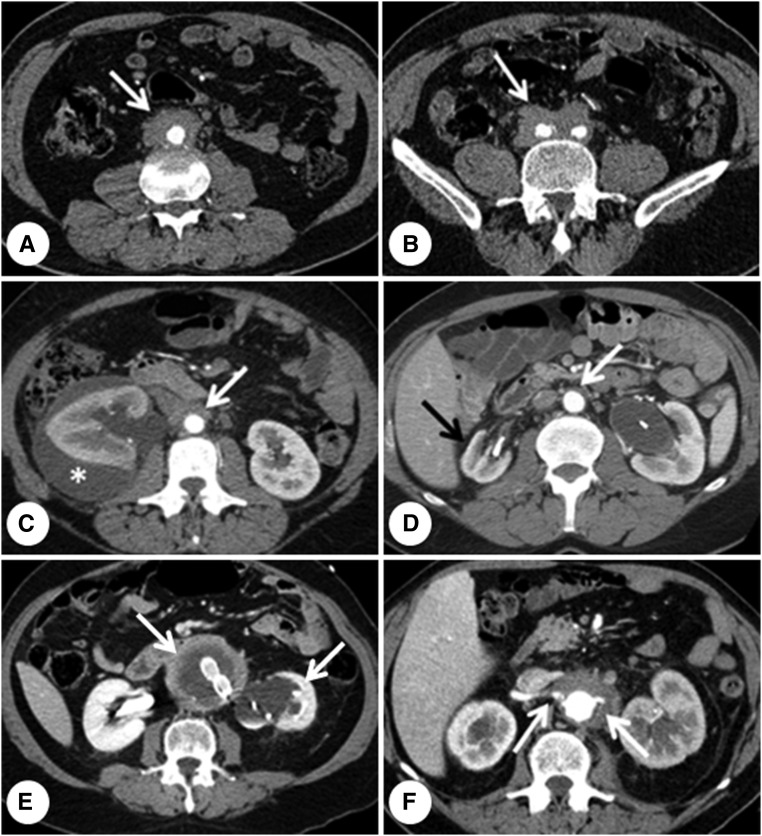
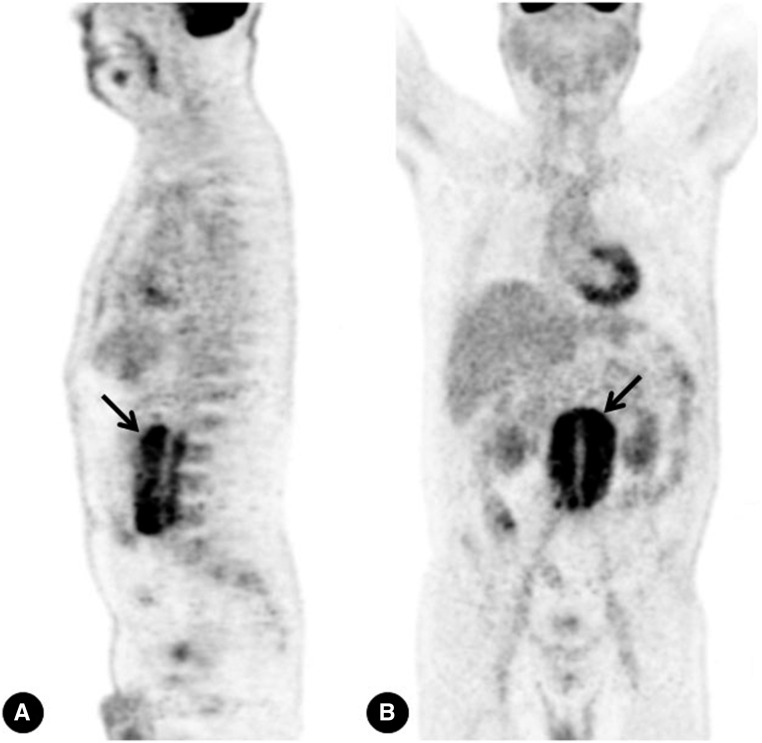
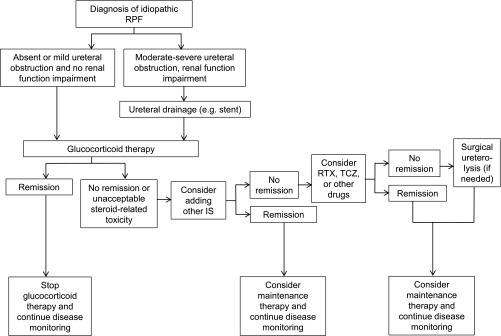
Idiopathic retroperitoneal fibrosis (RPF), reviewed herein, is a rare fibro-inflammatory disease that develops around the abdominal aorta and the iliac arteries, and spreads into the adjacent retroperitoneum, where it frequently causes ureteral obstruction and renal failure. The clinical phenotype of RPF is complex, because it can be associated with fibro-inflammatory disorders involving other organs, is considered part of the spectrum of IgG4-related disease, and often arises in patients with other autoimmune conditions. Obstructive uropathy is the most common complication, although other types of renal involvement may occur, including stenosis of the renal arteries and veins, renal atrophy, and different types of associated GN. Environmental and genetic factors contribute to disease susceptibility, whereas the immunopathogenesis of RPF is mediated by different immune cell types that eventually promote fibroblast activation. The diagnosis is made on the basis of computed tomography or magnetic resonance imaging, and positron emission tomography is a useful tool in disease staging and follow-up. Treatment of idiopathic RPF aims at relieving ureteral obstruction and inducing disease regression, and includes the use of glucocorticoids, combined or not with other traditional immunosuppressants. However, biologic therapies such as the B cell-depleting agent rituximab are emerging as potentially efficacious agents in difficult-to-treat cases.
Keywords: IgG4; fibrosis; hydronephrosis; retroperitoneal fibrosis; vasculitis.
Copyright © 2016 by the American Society of Nephrology.
Figures
References
-
- Vaglio A, Salvarani C, Buzio C: Retroperitoneal fibrosis. Lancet 367: 241–251, 2006 - PubMed
-
- van Bommel EF, Jansen I, Hendriksz TR, Aarnoudse AL: Idiopathic retroperitoneal fibrosis: prospective evaluation of incidence and clinicoradiologic presentation. Medicine (Baltimore) 88: 193–201, 2009 - PubMed
-
- Uibu T, Oksa P, Auvinen A, Honkanen E, Metsärinne K, Saha H, Uitti J, Roto P: Asbestos exposure as a risk factor for retroperitoneal fibrosis. Lancet 363: 1422–1426, 2004 - PubMed
-
- Vaglio A, Palmisano A, Alberici F, Maggiore U, Ferretti S, Cobelli R, Ferrozzi F, Corradi D, Salvarani C, Buzio C: Prednisone versus tamoxifen in patients with idiopathic retroperitoneal fibrosis: an open-label randomised controlled trial. Lancet 378: 338–346, 2011 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
