

Opportunities for Improvement in the Care of Patients Hospitalized for Inflammatory Bowel Disease-Related Colitis
- PMID: 26860508
- PMCID: PMC5716623
- DOI: 10.1007/s10620-016-4046-0
Opportunities for Improvement in the Care of Patients Hospitalized for Inflammatory Bowel Disease-Related Colitis
Abstract
Background: Algorithms for the diagnosis, management, and follow-up have been proposed for patients hospitalized for inflammatory bowel disease (IBD) colitis flare. The degree to which providers adhere to these algorithms is unknown. This study evaluated the quality of care in IBD patients hospitalized for disease-associated exacerbations and factors correlated with higher degrees of care.
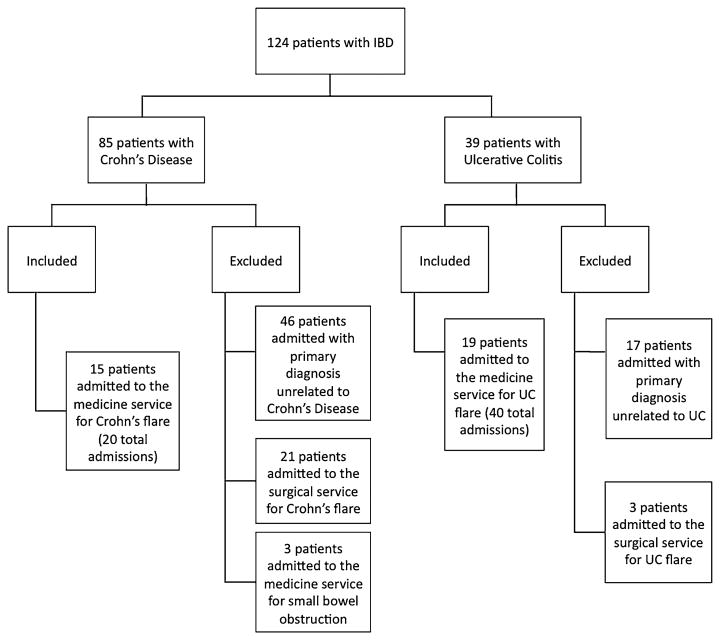
Methods: Retrospective chart review of 34 patients during 60 admissions to the medicine service for IBD colitis exacerbation between 2005 and 2012 at the Veterans Affairs San Diego Medical Center. Examined factors included laboratory testing, timing of consultation and intravenous steroids, abdominal imaging, endoscopic examination, venous thromboembolism (VTE) prophylaxis, narcotic use, Clostridium difficile and cytomegalovirus testing, symptomatology at discharge, timing of follow-up, and rates of readmission and mortality.
Results: Quality of care varied among the factors studied, ranging from 30.5 % for pharmacologic VTE prophylaxis to 84.7 % for gastroenterology consultation within 24 h. Of 60 admissions, 22 % were not tested for C. difficile. Fifteen percent of patients were discharged before meeting commonly used discharge criteria. Eighty percent were seen in clinic at any time post-discharge; 6.7 % were readmitted; 10 % were lost to follow-up; 1.7 % opted for outside follow-up; and 1.7 % expired.
Conclusions: The quality of care for patients admitted with IBD colitis flares is variable. These data outline opportunities for improvement, particularly in regard to pain management, VTE prophylaxis, and follow-up. Further studies are needed to test intervention strategies for practice improvement.
Keywords: Crohn’s disease; Inflammatory bowel disease; Quality indicators; Ulcerative colitis.
Conflict of interest statement
Similar articles
-
Quality of Care and Outcomes Among Hospitalized Inflammatory Bowel Disease Patients: A Multicenter Retrospective Study.Inflamm Bowel Dis. 2017 May;23(5):695-701. doi: 10.1097/MIB.0000000000001068. Inflamm Bowel Dis. 2017. PMID: 28426451
-
Risk factors for 90-day readmission in veterans with inflammatory bowel disease-Does post-discharge follow-up matter?Mil Med Res. 2018 Feb 8;5(1):5. doi: 10.1186/s40779-018-0153-x. Mil Med Res. 2018. PMID: 29502532 Free PMC article.
-
Nonattendance to gastroenterologist follow-up after discharge is associated with a thirty-days re-admission in patients with inflammatory bowel disease: a multicenter study.Minerva Med. 2021 Aug;112(4):467-473. doi: 10.23736/S0026-4806.21.07442-5. Epub 2021 Apr 21. Minerva Med. 2021. PMID: 33881281
-
Consensus statements on the risk, prevention, and treatment of venous thromboembolism in inflammatory bowel disease: Canadian Association of Gastroenterology.Gastroenterology. 2014 Mar;146(3):835-848.e6. doi: 10.1053/j.gastro.2014.01.042. Epub 2014 Jan 22. Gastroenterology. 2014. PMID: 24462530 Review.
-
Quality of care delivered to hospitalized inflammatory bowel disease patients.World J Gastroenterol. 2013 Oct 14;19(38):6360-6. doi: 10.3748/wjg.v19.i38.6360. World J Gastroenterol. 2013. PMID: 24151354 Free PMC article. Review.
Cited by
-
Day-by-Day Management of the Inpatient With Moderate to Severe Inflammatory Bowel Disease.Gastroenterol Hepatol (N Y). 2020 Sep;16(9):449-457. Gastroenterol Hepatol (N Y). 2020. PMID: 34035752 Free PMC article.
-
Bridges to excellence quality indicators in inflammatory bowel disease (IBD): differences between IBD and non-IBD gastroenterologists.Ann Gastroenterol. 2017;30(2):192-196. doi: 10.20524/aog.2016.0114. Epub 2016 Dec 16. Ann Gastroenterol. 2017. PMID: 28243040 Free PMC article.
-
Modern practical management of acute severe colitis.Indian J Gastroenterol. 2024 Feb;43(1):78-92. doi: 10.1007/s12664-024-01522-4. Epub 2024 Feb 26. Indian J Gastroenterol. 2024. PMID: 38407787 Review.
-
Vaccinating Patients With Inflammatory Bowel Disease.Gastroenterol Hepatol (N Y). 2016 Sep;12(9):540-546. Gastroenterol Hepatol (N Y). 2016. PMID: 27917091 Free PMC article.
-
Practice pattern variability in the management of acute severe colitis: a UK provider survey.Frontline Gastroenterol. 2019 Aug 17;11(4):272-279. doi: 10.1136/flgastro-2019-101277. eCollection 2020. Frontline Gastroenterol. 2019. PMID: 32587670 Free PMC article.
References
-
- Danese S, Fiocchi C. Ulcerative colitis. N Engl J Med. 2011;365:1713–1725. - PubMed
-
- Gunnarsson C, Chen J, Rizzo JA, Ladapo JA, Naim A, Lofland JH. The employee absenteeism costs of inflammatory bowel disease: evidence from US National Survey Data. J Occup Environ Med. 2013;55:393–401. - PubMed
-
- Murthy SK, Steinhart AH, Tinmouth J, Austin PC, Nguyen GC. Impact of gastroenterologist care on health outcomes of hospitalised ulcerative colitis patients. Gut. 2012;61:1410–1416. - PubMed
-
- Cohen RD, Yu AP, Wu EQ, Xie J, Mulani PM, Chao J. Systematic review: the costs of ulcerative colitis in Western countries. Aliment Pharmacol Ther. 2010;31:693–707. - PubMed
-
- van Langenberg DR, Simon SB, Holtmann GJ, Andrews JM. The burden of inpatient costs in inflammatory bowel disease and opportunities to optimize care: a single metropolitan Australian center experience. J Crohn's Colitis. 2010;4:413–421. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
