

Effect of ICU strain on timing of limitations in life-sustaining therapy and on death
- PMID: 26862018
- PMCID: PMC4846491
- DOI: 10.1007/s00134-016-4240-8
Effect of ICU strain on timing of limitations in life-sustaining therapy and on death
Abstract
Purpose: The effect of capacity strain in an ICU on the timing of end-of-life decision-making is unknown. We sought to determine how changes in strain impact timing of new do-not-resuscitate (DNR) orders and of death.
Methods: Retrospective cohort study of 9891 patients dying in the hospital following an ICU stay ≥72 h in Project IMPACT, 2001-2008. We examined the effect of ICU capacity strain (measured by standardized census, proportion of new admissions, and average patient acuity) on time to initiation of DNR orders and time to death for all ICU decedents using fixed-effects linear regression.
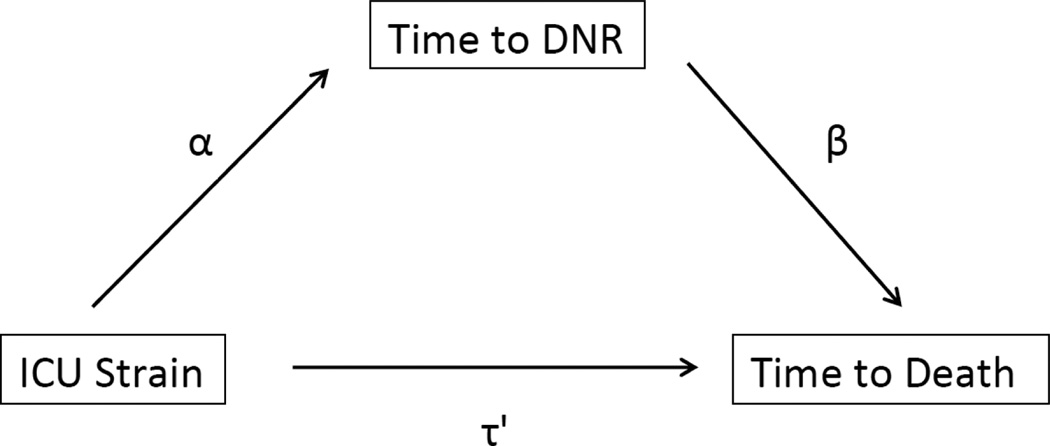
Results: Increases in strain were associated with shorter time to DNR for patients with limitations in therapy (predicted time to DNR 6.11 days for highest versus 7.70 days for lowest quintile of acuity, p = 0.02; 6.50 days for highest versus 7.77 days for lowest quintile of admissions, p < 0.001), and shorter time to death (predicted time to death 7.64 days for highest versus 9.05 days for lowest quintile of admissions, p < 0.001; 8.28 days for highest versus 9.06 days for lowest quintile of census, only in closed ICUs, p = 0.006). Time to DNR order significantly mediated relationships between acuity and admissions and time to death, explaining the entire effect of acuity, and 65 % of the effect of admissions. There was no association between strain and time to death for decedents without a limitation in therapy.
Conclusions: Strains in ICU capacity are associated with end-of-life decision-making, with shorter times to placement of DNR orders and death for patients admitted during high-strain days.
Keywords: Critical care; Decision-making; End-of-life care; Palliative care.
Conflict of interest statement
May Hua reported no conflicts of interest.
Scott Halpern reported no conflicts of interest.
Nicole Gabler reported no conflicts of interest.
Hannah Wunsch reported no conflicts of interest.
Figures
Comment in
-
Intensive care unit strain should not rush physicians into making inappropriate decisions, but merely reduce the time to the right decisions being made.Ann Transl Med. 2016 Aug;4(16):316. doi: 10.21037/atm.2016.07.27. Ann Transl Med. 2016. PMID: 27668236 Free PMC article. No abstract available.
References
-
- Garland A, Connors AF. Physicians' influence over decisions to forego life support. J Palliat Med. 2007;10:1298–1305. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
