

The 'pit-crew' model for improving door-to-needle times in endovascular stroke therapy: a Six-Sigma project
- PMID: 26863106
- PMCID: PMC4853568
- DOI: 10.1136/neurintsurg-2015-012219
The 'pit-crew' model for improving door-to-needle times in endovascular stroke therapy: a Six-Sigma project
Abstract
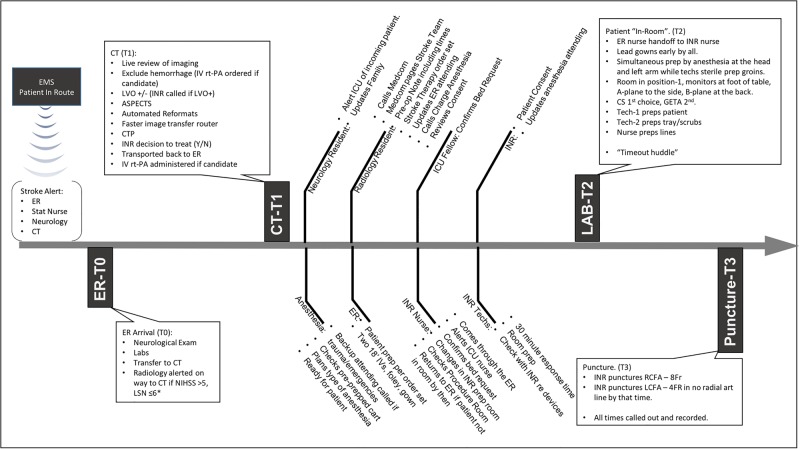
Background: Delays in delivering endovascular stroke therapy adversely affect outcomes. Time-sensitive treatments such as stroke interventions benefit from methodically developed protocols. Clearly defined roles in these protocols allow for parallel processing of tasks, resulting in consistent delivery of care.
Objective: To present the outcomes of a quality-improvement (QI) process directed at reducing stroke treatment times in a tertiary level academic medical center.
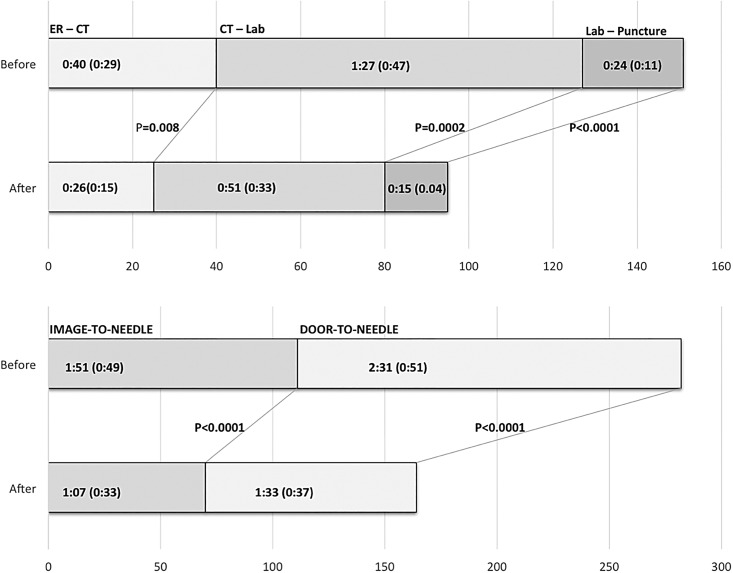
Methods: A Six-Sigma-based QI process was developed over a 3-month period. After an initial analysis, procedures were implemented and fine-tuned to identify and address rate-limiting steps in the endovascular care pathway. Prospectively recorded treatment times were then compared in two groups of patients who were treated 'before' (n=64) or 'after' (n=30) the QI process. Three time intervals were measured: emergency room (ER) to arrival for CT scan (ER-CT), CT scan to interventional laboratory arrival (CT-Lab), and interventional laboratory arrival to groin puncture (Lab-puncture).
Results: The ER-CT time was 40 (±29) min in the 'before' and 26 (±15) min in the 'after' group (p=0.008). The CT-Lab time was 87 (±47) min in the 'before' and 51 (±33) min in the 'after' group (p=0.0002). The Lab-puncture time was 24 (±11) min in the 'before' and 15 (±4) min in the 'after' group (p<0.0001). The overall ER-arrival to groin-puncture time was reduced from 2 h, 31 min (±51) min in the 'before' to 1 h, 33 min (±37) min in the 'after' group, (p<0.0001). The improved times were seen for both working hours and off-hours interventions.
Conclusions: A protocol-driven process can significantly improve efficiency of care in time-sensitive stroke interventions.
Keywords: Standards; Stroke.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://www.bmj.com/company/products-services/rights-and-licensing/
Figures
References
-
- Powers WJ, Derdeyn CP, Biller J, et al. . 2015 American Heart Association/American Stroke Association focused update of the 2013 guidelines for the early management of patients with acute ischemic stroke regarding endovascular treatment: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 2015;46:3020–35. 10.1161/STR.0000000000000074 - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous