

Long-Term Safety and Efficacy of Lowering Low-Density Lipoprotein Cholesterol With Statin Therapy: 20-Year Follow-Up of West of Scotland Coronary Prevention Study
- PMID: 26864092
- PMCID: PMC4894764
- DOI: 10.1161/CIRCULATIONAHA.115.019014
Long-Term Safety and Efficacy of Lowering Low-Density Lipoprotein Cholesterol With Statin Therapy: 20-Year Follow-Up of West of Scotland Coronary Prevention Study
Abstract
Background: Extended follow-up of statin-based low-density lipoprotein cholesterol lowering trials improves the understanding of statin safety and efficacy. Examining cumulative cardiovascular events (total burden of disease) gives a better appreciation of the clinical value of statins. This article evaluates the long-term impact of therapy on mortality and cumulative morbidity in a high-risk cohort of men.
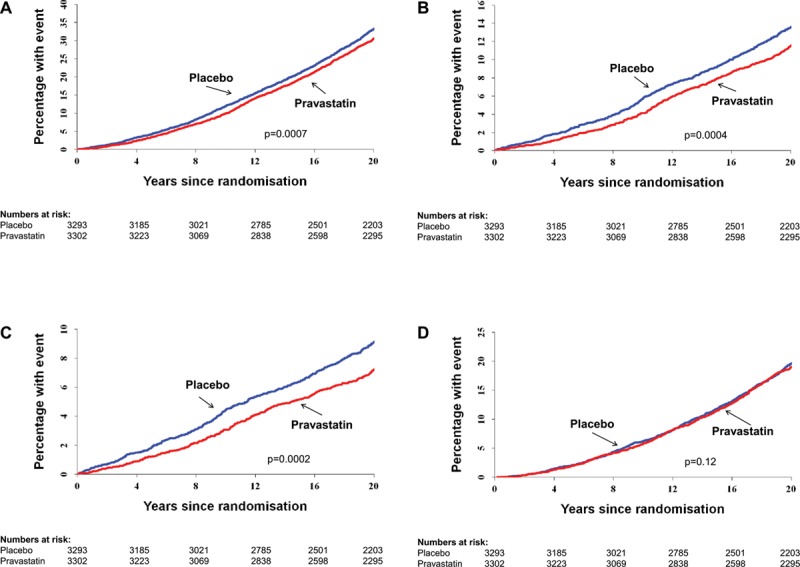
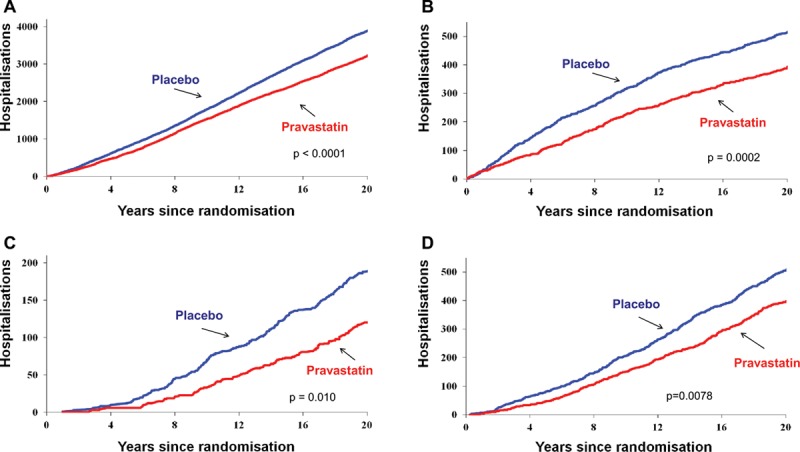
Methods and results: The West of Scotland Coronary Prevention Study was a primary prevention trial in 45- to 64-year-old men with high low-density lipoprotein cholesterol. A total of 6595 men were randomized to receive pravastatin 40 mg once daily or placebo for an average of 4.9 years. Subsequent linkage to electronic health records permitted analysis of major incident events over 20 years. Post trial statin use was recorded for 5 years after the trial but not for the last 10 years. Men allocated to pravastatin had reduced all-cause mortality (hazard ratio, 0.87; 95% confidence interval, 0.80-0.94; P=0.0007), attributable mainly to a 21% decrease in cardiovascular death (hazard ratio, 0.79; 95% confidence interval, 0.69-0.90; P=0.0004). There was no difference in noncardiovascular or cancer death rates between groups. Cumulative hospitalization event rates were lower in the statin-treated arm: by 18% for any coronary event (P=0.002), by 24% for myocardial infarction (P=0.01), and by 35% for heart failure (P=0.002). There were no significant differences between groups in hospitalization for noncardiovascular causes.
Conclusion: Statin treatment for 5 years was associated with a legacy benefit, with improved survival and a substantial reduction in cardiovascular disease outcomes over a 20-year period, supporting the wider adoption of primary prevention strategies.
Keywords: clinical trial [publication type]; coronary disease; heart failure; primary prevention; safety.
© 2016 The Authors.
Figures
Comment in
-
Reducing exposure to cardiovascular risk factors: the legacy of prevention.J Thorac Dis. 2016 Sep;8(9):2340-2343. doi: 10.21037/jtd.2016.08.83. J Thorac Dis. 2016. PMID: 27746971 Free PMC article. No abstract available.
-
Choosing between percutaneous coronary intervention and coronary artery bypass graft surgery for nondiabetic patients with multivessel disease.J Thorac Dis. 2016 Nov;8(11):3028-3033. doi: 10.21037/jtd.2016.11.104. J Thorac Dis. 2016. PMID: 28066575 Free PMC article. No abstract available.
-
Investigating the long-term legacy of statin therapy.J Thorac Dis. 2017 Apr;9(4):936-939. doi: 10.21037/jtd.2017.03.10. J Thorac Dis. 2017. PMID: 28523141 Free PMC article. No abstract available.
References
-
- Stone NJ, Robinson JG, Lichtenstein AH, Bairey Merz CN, Blum CB, Eckel RH, Goldberg AC, Gordon D, Levy D, Lloyd-Jones DM, McBride P, Schwartz JS, Shero ST, Smith SC, Jr, Watson K, Wilson PW, Eddleman KM, Jarrett NM, LaBresh K, Nevo L, Wnek J, Anderson JL, Halperin JL, Albert NM, Bozkurt B, Brindis RG, Curtis LH, DeMets D, Hochman JS, Kovacs RJ, Ohman EM, Pressler SJ, Sellke FW, Shen WK, Smith SC, Jr, Tomaselli GF American College of Cardiology/American Heart Association Task Force on Practice Guidelines. 2013 ACC/AHA guideline on the treatment of blood cholesterol to reduce atherosclerotic cardiovascular risk in adults: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation. 2014;129(suppl 2):S1–S45. doi: 10.1161/01.cir.0000437738.63853.7a. - PubMed
-
- Perk J, De Backer G, Gohlke H, Graham I, Reiner Z, Verschuren M, Albus C, Benlian P, Boysen G, Cifkova R, Deaton C, Ebrahim S, Fisher M, Germano G, Hobbs R, Hoes A, Karadeniz S, Mezzani A, Prescott E, Ryden L, Scherer M, Syvänne M, Scholte op Reimer WJ, Vrints C, Wood D, Zamorano JL, Zannad F European Association for Cardiovascular Prevention & Rehabilitation (EACPR); ESC Committee for Practice Guidelines (CPG) European guidelines on cardiovascular disease prevention in clinical practice (version 2012): the Fifth Joint Task Force of the European Society of Cardiology and Other Societies on Cardiovascular Disease Prevention in Clinical Practice (constituted by representatives of nine societies and by invited experts). Eur Heart J. 2012;33:1635–1701. doi: 10.1093/eurheartj/ehs092. - PubMed
-
- D’Agostino RB, Sr, Ansell BJ, Mora S, Krumholz HM. The guidelines battle on starting statins. N Engl J Med. 2014;370:1652–1658. doi: 10.1056/NEJMclde1314766. - PubMed
-
- Redberg RF, Katz MH. Healthy men should not take statins. JAMA. 2012;307:1491–1492. doi: 10.1001/jama.2012.423. - PubMed
-
- Taylor FC, Huffman M, Ebrahim S. Statin therapy for primary prevention of cardiovascular disease. JAMA. 2013;310:2451–2452. doi: 10.1001/jama.2013.281348. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
