

Effect of Behavioral Interventions on Inappropriate Antibiotic Prescribing Among Primary Care Practices: A Randomized Clinical Trial
- PMID: 26864410
- PMCID: PMC6689234
- DOI: 10.1001/jama.2016.0275
Effect of Behavioral Interventions on Inappropriate Antibiotic Prescribing Among Primary Care Practices: A Randomized Clinical Trial
Abstract
Importance: Interventions based on behavioral science might reduce inappropriate antibiotic prescribing.
Objective: To assess effects of behavioral interventions and rates of inappropriate (not guideline-concordant) antibiotic prescribing during ambulatory visits for acute respiratory tract infections.
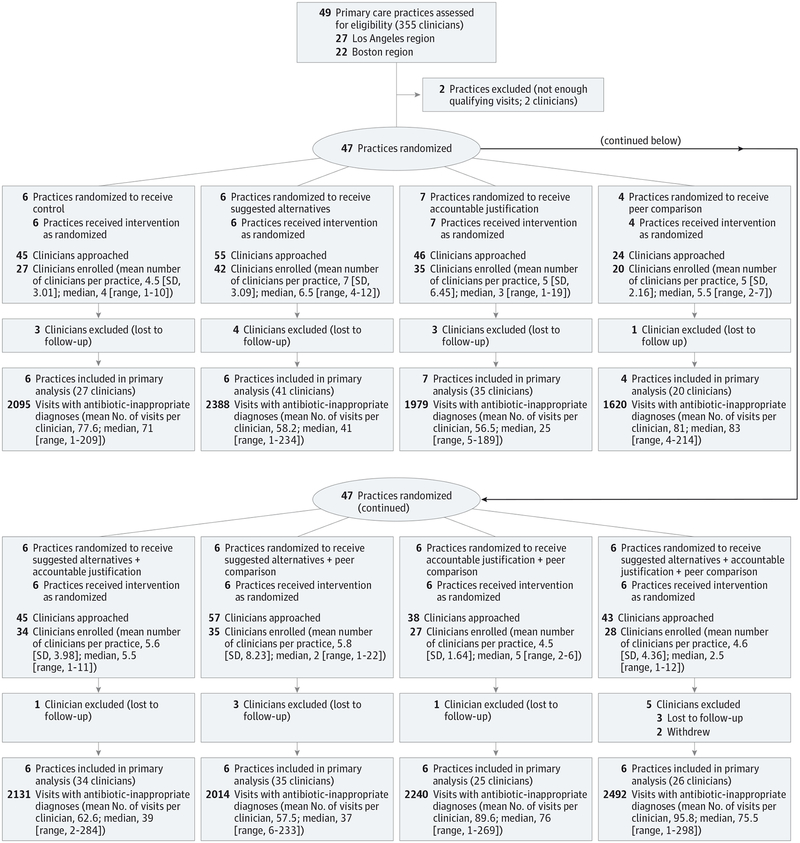
Design, setting, and participants: Cluster randomized clinical trial conducted among 47 primary care practices in Boston and Los Angeles. Participants were 248 enrolled clinicians randomized to receive 0, 1, 2, or 3 interventions for 18 months. All clinicians received education on antibiotic prescribing guidelines on enrollment. Interventions began between November 1, 2011, and October 1, 2012. Follow-up for the latest-starting sites ended on April 1, 2014. Adult patients with comorbidities and concomitant infections were excluded.
Interventions: Three behavioral interventions, implemented alone or in combination: suggested alternatives presented electronic order sets suggesting nonantibiotic treatments; accountable justification prompted clinicians to enter free-text justifications for prescribing antibiotics into patients' electronic health records; peer comparison sent emails to clinicians that compared their antibiotic prescribing rates with those of "top performers" (those with the lowest inappropriate prescribing rates).
Main outcomes and measures: Antibiotic prescribing rates for visits with antibiotic-inappropriate diagnoses (nonspecific upper respiratory tract infections, acute bronchitis, and influenza) from 18 months preintervention to 18 months afterward, adjusting each intervention's effects for co-occurring interventions and preintervention trends, with random effects for practices and clinicians.
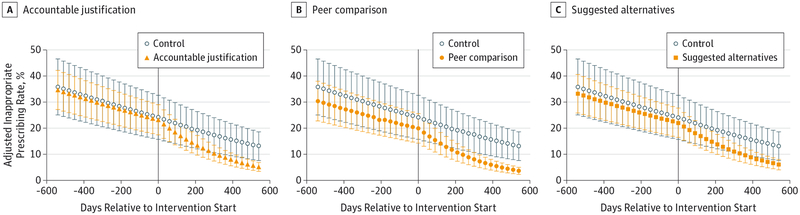
Results: There were 14,753 visits (mean patient age, 47 years; 69% women) for antibiotic-inappropriate acute respiratory tract infections during the baseline period and 16,959 visits (mean patient age, 48 years; 67% women) during the intervention period. Mean antibiotic prescribing rates decreased from 24.1% at intervention start to 13.1% at intervention month 18 (absolute difference, -11.0%) for control practices; from 22.1% to 6.1% (absolute difference, -16.0%) for suggested alternatives (difference in differences, -5.0% [95% CI, -7.8% to 0.1%]; P = .66 for differences in trajectories); from 23.2% to 5.2% (absolute difference, -18.1%) for accountable justification (difference in differences, -7.0% [95% CI, -9.1% to -2.9%]; P < .001); and from 19.9% to 3.7% (absolute difference, -16.3%) for peer comparison (difference in differences, -5.2% [95% CI, -6.9% to -1.6%]; P < .001). There were no statistically significant interactions (neither synergy nor interference) between interventions.
Conclusions and relevance: Among primary care practices, the use of accountable justification and peer comparison as behavioral interventions resulted in lower rates of inappropriate antibiotic prescribing for acute respiratory tract infections.
Trial registration: clinicaltrials.gov Identifier: NCT01454947.
Conflict of interest statement
Figures
Comment in
-
Improving Outpatient Antibiotic Prescribing: Another Nudge in the Right Direction.JAMA. 2016 Feb 9;315(6):558-9. doi: 10.1001/jama.2016.0430. JAMA. 2016. PMID: 26864408 No abstract available.
References
-
- Tackling a Crisis for the Future Health and Wealth of Nations. Review on Antimicrobial Resistance website. http://amr-review.org/. December 2014. Accessed January 14, 2016.
-
- Office of the Press Secretary, The White House. Executive Order—Combating Antibiotic-Resistant Bacteria. Whitehouse.gov; website; https://www.whitehouse.gov/the-press-office/2014/09/18/executive-order-c.... 2014. Accessed January 14, 2016.
-
- Steinman MA, Gonzales R, Linder JA, Landefeld CS. Changing use of antibiotics in community-based outpatient practice, 1991–1999. Ann Intern Med. 2003;138(7):525–533. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
