

Composition and dynamics of the respiratory tract microbiome in intubated patients
- PMID: 26865050
- PMCID: PMC4750361
- DOI: 10.1186/s40168-016-0151-8
Composition and dynamics of the respiratory tract microbiome in intubated patients
Abstract
Background: Lower respiratory tract infection (LRTI) is a major contributor to respiratory failure requiring intubation and mechanical ventilation. LRTI also occurs during mechanical ventilation, increasing the morbidity and mortality of intubated patients. We sought to understand the dynamics of respiratory tract microbiota following intubation and the relationship between microbial community structure and infection.
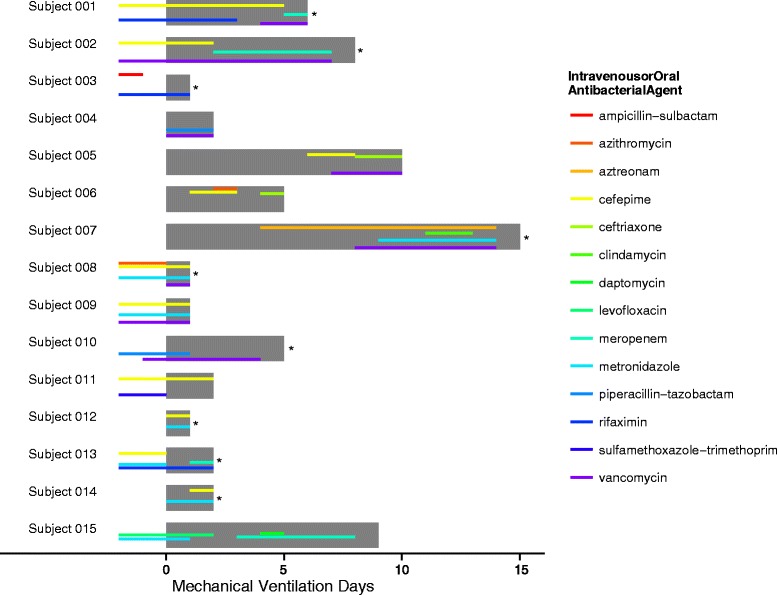
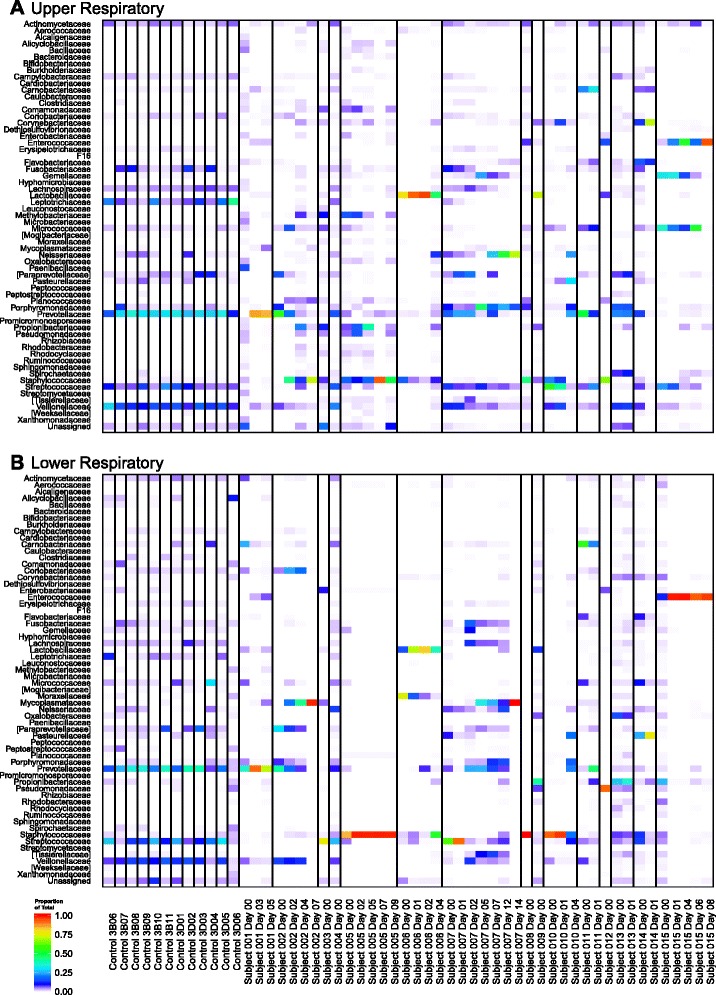
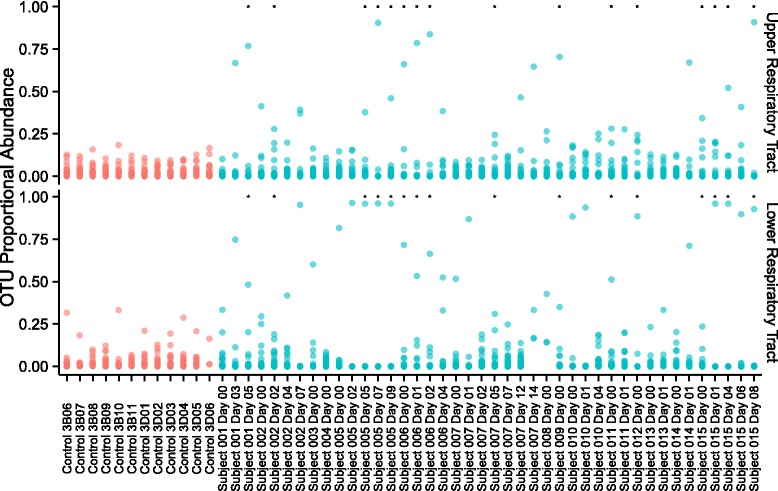
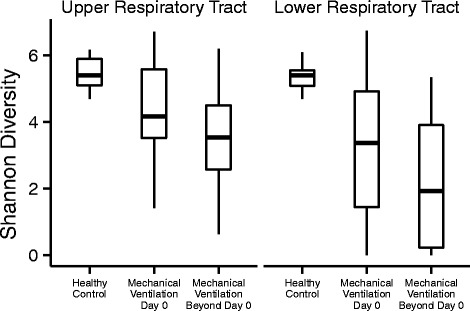
Results: We enrolled a cohort of 15 subjects with respiratory failure requiring intubation and mechanical ventilation from the medical intensive care unit at an academic medical center. Oropharyngeal (OP) and deep endotracheal (ET) secretions were sampled within 24 h of intubation and every 48-72 h thereafter. Bacterial community profiling was carried out by purifying DNA, PCR amplification of 16S ribosomal RNA (rRNA) gene sequences, deep sequencing, and bioinformatic community analysis. We compared enrolled subjects to a cohort of healthy subjects who had lower respiratory tract sampling by bronchoscopy. In contrast to the diverse upper respiratory tract and lower respiratory tract microbiota found in healthy controls, critically ill subjects had lower initial diversity at both sites. Diversity further diminished over time on the ventilator. In several subjects, the bacterial community was dominated by a single taxon over multiple time points. The clinical diagnosis of LRTI ascertained by chart review correlated with low community diversity and dominance of a single taxon. Dominant taxa matched clinical bacterial cultures where cultures were obtained and positive. In several cases, dominant taxa included bacteria not detected by culture, including Ureaplasma parvum and Enterococcus faecalis.
Conclusions: Longitudinal analysis of respiratory tract microbiota in critically ill patients provides insight into the pathogenesis and diagnosis of LRTI. 16S rRNA gene sequencing of endotracheal aspirate samples holds promise for expanded pathogen identification.
Figures
References
-
- Niederman MS, Mandell LA, Anzueto A, Bass JB, Broughton WA, Campbell GD, et al. Guidelines for the management of adults with community-acquired pneumonia. Diagnosis, assessment of severity, antimicrobial therapy, and prevention. Am J Respir Crit Care Med. 2001;163:1730–54. doi: 10.1164/ajrccm.163.7.at1010. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
