

Basic FGF or VEGF gene therapy corrects insufficiency in the intrinsic healing capacity of tendons
- PMID: 26865366
- PMCID: PMC4749961
- DOI: 10.1038/srep20643
Basic FGF or VEGF gene therapy corrects insufficiency in the intrinsic healing capacity of tendons
Abstract
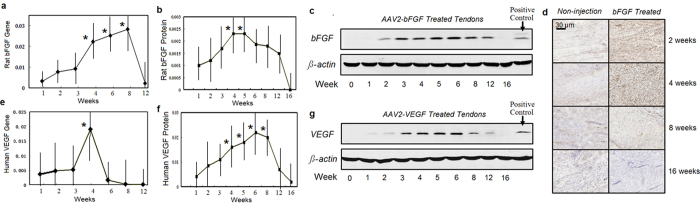
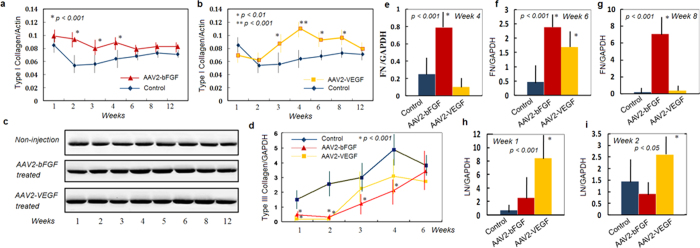
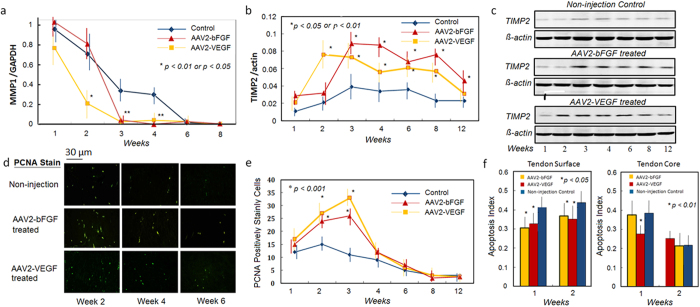
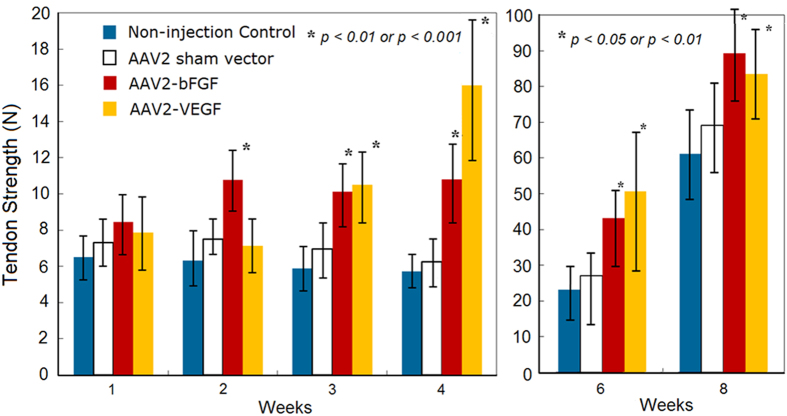
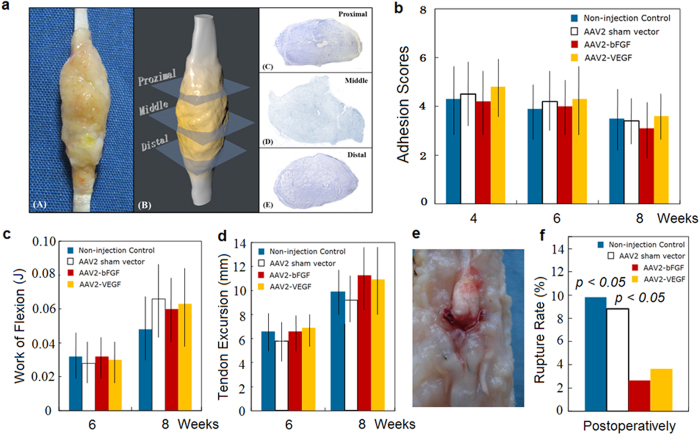
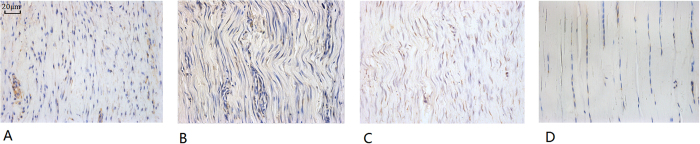
Tendon injury during limb motion is common. Damaged tendons heal poorly and frequently undergo unpredictable ruptures or impaired motion due to insufficient innate healing capacity. By basic fibroblast growth factor (bFGF) or vascular endothelial growth factor (VEGF) gene therapy via adeno-associated viral type-2 (AAV2) vector to produce supernormal amount of bFGF or VEGF intrinsically in the tendon, we effectively corrected the insufficiency of the tendon healing capacity. This therapeutic approach (1) resulted in substantial amelioration of the low growth factor activity with significant increases in bFGF or VEGF from weeks 4 to 6 in the treated tendons (p < 0.05 or p < 0.01), (2) significantly promoted production of type I collagen and other extracellular molecules (p < 0.01) and accelerated cellular proliferation, and (3) significantly increased tendon strength by 68-91% from week 2 after AAV2-bFGF treatment and by 82-210% from week 3 after AAV2-VEGF compared with that of the controls (p < 0.05 or p < 0.01). Moreover, the transgene expression dissipated after healing was complete. These findings show that the gene transfers provide an optimistic solution to the insufficiencies of the intrinsic healing capacity of the tendon and offers an effective therapeutic possibility for patients with tendon disunion.
Conflict of interest statement
The authors declare no competing financial interests.
Figures
Similar articles
-
Tendon healing in vitro: bFGF gene transfer to tenocytes by adeno-associated viral vectors promotes expression of collagen genes.J Hand Surg Am. 2005 Nov;30(6):1255-61. doi: 10.1016/j.jhsa.2005.06.001. J Hand Surg Am. 2005. PMID: 16344185
-
Adeno-associated virus-2-mediated bFGF gene transfer to digital flexor tendons significantly increases healing strength. an in vivo study.J Bone Joint Surg Am. 2008 May;90(5):1078-89. doi: 10.2106/JBJS.F.01188. J Bone Joint Surg Am. 2008. PMID: 18451401
-
Modulation of digital flexor tendon healing by vascular endothelial growth factor gene transfection in a chicken model.Gene Ther. 2017 Apr;24(4):234-240. doi: 10.1038/gt.2017.12. Epub 2017 Feb 21. Gene Ther. 2017. PMID: 28221337
-
Gene therapy strategies to improve strength and quality of flexor tendon healing.Expert Opin Biol Ther. 2016;16(3):291-301. doi: 10.1517/14712598.2016.1134479. Epub 2016 Feb 6. Expert Opin Biol Ther. 2016. PMID: 26853840 Review.
-
The roles of growth factors in tendon and ligament healing.Sports Med. 2003;33(5):381-94. doi: 10.2165/00007256-200333050-00004. Sports Med. 2003. PMID: 12696985 Review.
Cited by
-
Modulation of vascular response after injury in the rat Achilles tendon alters healing capacity.J Orthop Res. 2021 Sep;39(9):2000-2016. doi: 10.1002/jor.24861. Epub 2020 Oct 1. J Orthop Res. 2021. PMID: 32936495 Free PMC article.
-
Autologous Microfragmented Adipose Tissue Reduces the Catabolic and Fibrosis Response in an In Vitro Model of Tendon Cell Inflammation.Stem Cells Int. 2019 Dec 5;2019:5620286. doi: 10.1155/2019/5620286. eCollection 2019. Stem Cells Int. 2019. PMID: 31885616 Free PMC article.
-
Tumour necrosis factor alpha, interleukin 1 beta and interferon gamma have detrimental effects on equine tenocytes that cannot be rescued by IL-1RA or mesenchymal stromal cell-derived factors.Cell Tissue Res. 2023 Mar;391(3):523-544. doi: 10.1007/s00441-022-03726-6. Epub 2022 Dec 22. Cell Tissue Res. 2023. PMID: 36543895 Free PMC article.
-
The Functions and Mechanisms of Basic Fibroblast Growth Factor in Tendon Repair.Front Physiol. 2022 Jun 13;13:852795. doi: 10.3389/fphys.2022.852795. eCollection 2022. Front Physiol. 2022. PMID: 35770188 Free PMC article. Review.
-
Bio-artificial pleura using autologous dermal fibroblast sheets to mitigate air leaks during thoracoscopic lung resection.NPJ Regen Med. 2021 Jan 4;6(1):2. doi: 10.1038/s41536-020-00113-z. NPJ Regen Med. 2021. PMID: 33398054 Free PMC article.
References
-
- Clayton R. A. & Court-Brown C. M. The epidemiology of musculoskeletal tendinous and ligamentous injuries. Injury. 39, 1338–1344 (2008). - PubMed
-
- Pennisi E. Tending tender tendons. Science. 295 (5557), 1011 (2002). - PubMed
-
- Beredjiklian P. K. Biological aspects of flexor tendon laceration and repair. J Bone Joint Surg (Am). 85, 539–550 (2003). - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
