

Long-term safety and efficacy of teriflunomide: Nine-year follow-up of the randomized TEMSO study
- PMID: 26865517
- PMCID: PMC4782117
- DOI: 10.1212/WNL.0000000000002441
Long-term safety and efficacy of teriflunomide: Nine-year follow-up of the randomized TEMSO study
Erratum in
-
Long-term safety and efficacy of teriflunomide: Nine-year follow-up of the randomized TEMSO study.Neurology. 2016 Oct 4;87(14):1524. doi: 10.1212/WNL.0000000000003219. Neurology. 2016. PMID: 27698155 Free PMC article. No abstract available.
Abstract
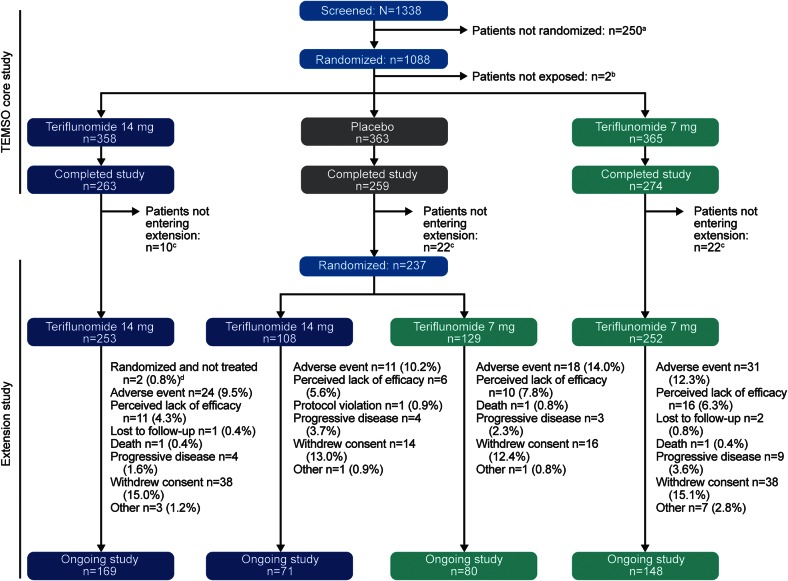
Objective: To report safety and efficacy outcomes from up to 9 years of treatment with teriflunomide in an extension (NCT00803049) of the pivotal phase 3 Teriflunomide Multiple Sclerosis Oral (TEMSO) trial (NCT00134563).
Methods: A total of 742 patients entered the extension. Teriflunomide-treated patients continued the original dose; those previously receiving placebo were randomized 1:1 to teriflunomide 14 mg or 7 mg.
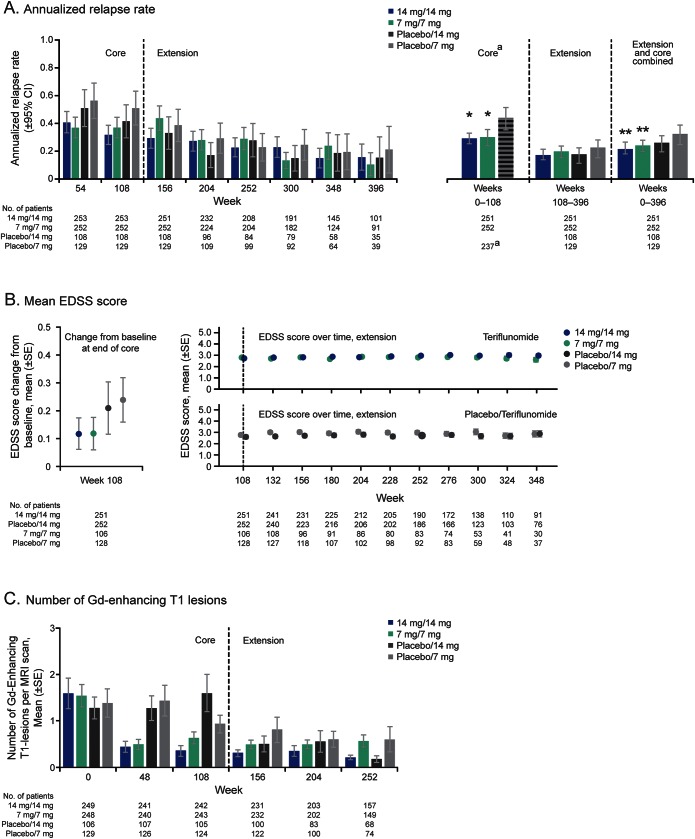
Results: By June 2013, median (maximum) teriflunomide exposure exceeded 190 (325) weeks per patient; 468 patients (63%) remained on treatment. Teriflunomide was well-tolerated with continued exposure. The most common adverse events (AEs) matched those in the core study. In extension year 1, first AEs of transient liver enzyme increases or reversible hair thinning were generally attributable to patients switching from placebo to teriflunomide. Approximately 11% of patients discontinued treatment owing to AEs. Twenty percent of patients experienced serious AEs. There were 3 deaths unrelated to teriflunomide. Soon after the extension started, annualized relapse rates and gadolinium-enhancing T1 lesion counts fell in patients switching from placebo to teriflunomide, remaining low thereafter. Disability remained stable in all treatment groups (median Expanded Disability Status Scale score ≤2.5; probability of 12-week disability progression ≤0.48).
Conclusions: In the TEMSO extension, safety observations were consistent with the core trial, with no new or unexpected AEs in patients receiving teriflunomide for up to 9 years. Disease activity decreased in patients switching from placebo and remained low in patients continuing on teriflunomide.
Classification of evidence: This study provides Class III evidence that long-term treatment with teriflunomide is well-tolerated and efficacy of teriflunomide is maintained long-term.
© 2016 American Academy of Neurology.
Figures
References
-
- O'Connor PW, Li D, Freedman MS, et al. A phase II study of the safety and efficacy of teriflunomide in multiple sclerosis with relapses. Neurology 2006;66:894–900. - PubMed
-
- O'Connor P, Wolinsky JS, Confavreux C, et al. Randomized trial of oral teriflunomide for relapsing multiple sclerosis. N Engl J Med 2011;365:1293–1303. - PubMed
-
- Confavreux C, O'Connor P, Comi G, et al. Oral teriflunomide for patients with relapsing multiple sclerosis (TOWER): a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Neurol 2014;13:247–256. - PubMed
-
- Vermersch P, Czlonkowska A, Grimaldi LM, et al. Teriflunomide versus subcutaneous interferon beta-1a in patients with relapsing multiple sclerosis: a randomised, controlled phase 3 trial. Mult Scler 2014;20:705–716. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials