

Transpapillary drainage of walled-off pancreatic necrosis - a single center experience
- PMID: 26865888
- PMCID: PMC4729724
- DOI: 10.5114/wiitm.2015.55677
Transpapillary drainage of walled-off pancreatic necrosis - a single center experience
Abstract
Introduction: Walled-off pancreatic necrosis (WOPN) often coexists with disruption of the main pancreatic duct that manifests as a leak of contrast medium into the necrotic collection during endoscopic retrograde pancreatography.
Aim: To assess the efficacy and safety of treatment of patients with symptomatic WOPN and disruption of the main pancreatic duct, who underwent endoscopic transpapillary drainage as the only access to the necrosis cavity.
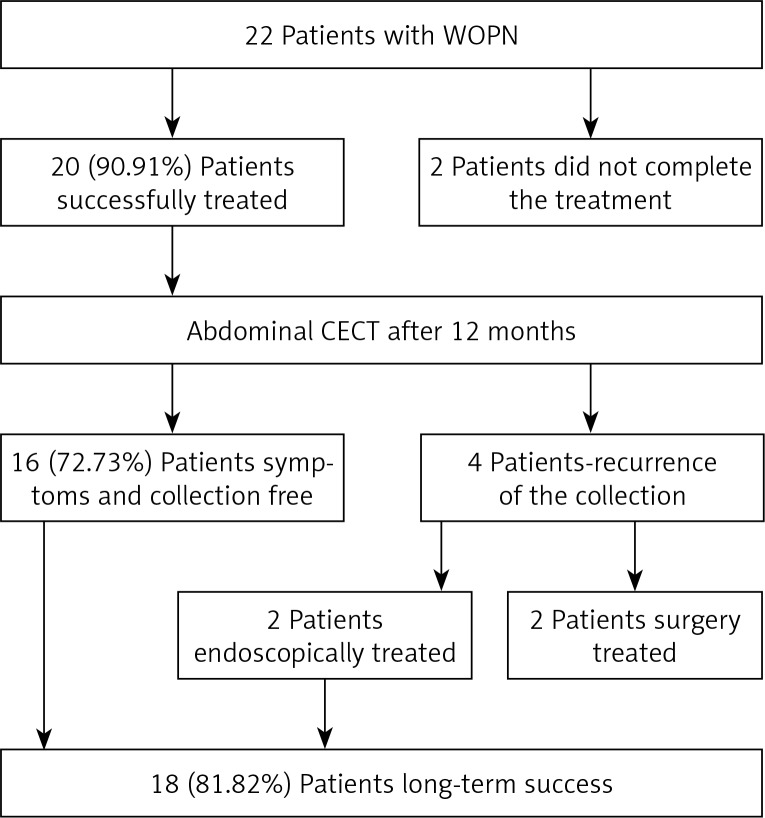
Material and methods: In 22 patients with symptomatic WOPN, active endoscopic transpapillary drainage was performed. During endoscopic retrograde pancreatography (ERP), partial disruption of the main pancreatic duct was observed in 14 patients and complete disruption in 8 patients. After the active drainage was finished, a transpapillary pancreatic stent was inserted into the main pancreatic duct, which was later exchanged after 6, 12 and 24 months or when no extravasation of contrast from the pancreatic duct was observed. The results of treatment and complications were compared retrospectively.
Results: The mean duration of active drainage was 22 (range: 7-94) days. Complications of endotherapy occurred in 3/22 patients. The mean time of the main pancreatic duct stenting was 304 (range: 85-519) days. Success of endoscopic treatment of WOPN and pancreatic duct disruption was achieved in 20/22 patients. During a 1-year follow-up, recurrence of the collection was noted in 4/20 patients. Long-term success was achieved in 16/22 patients.
Conclusions: In patients with WOPN who cannot undergo transmural drainage when there is a communication between the necrotic collection and the main pancreatic duct, transpapillary access may be an effective and safe method of treatment.
Keywords: acute pancreatitis; disconnected pancreatic duct syndrome; endoscopic drainage/debridement; transpapillary drainage/debridement; walled-off pancreatic necrosis.
Figures


Similar articles
-
Endoscopic transpapillary drainage for walled-off pancreatic necrosis with complete main pancreatic duct disruption by metallic stent placement: A retrospective study.Front Med (Lausanne). 2022 Dec 7;9:1064463. doi: 10.3389/fmed.2022.1064463. eCollection 2022. Front Med (Lausanne). 2022. PMID: 36569130 Free PMC article.
-
The role of endoscopic treatment of pancreatic duct disruption in patients with walled-off pancreatic necrosis.Surg Endosc. 2018 Dec;32(12):4939-4952. doi: 10.1007/s00464-018-6255-4. Epub 2018 Jun 4. Surg Endosc. 2018. PMID: 29869080
-
The Role of Endoscopic Transpapillary Stenting of the Main Pancreatic Duct during the Endoscopic Treatment of Pancreatic Fluid Collections.J Clin Med. 2021 Feb 14;10(4):761. doi: 10.3390/jcm10040761. J Clin Med. 2021. PMID: 33672814 Free PMC article. Review.
-
Endoscopic treatment of walled-off pancreatic necrosis complicated with pancreaticocolonic fistula.Surg Endosc. 2018 Mar;32(3):1572-1580. doi: 10.1007/s00464-018-6032-4. Epub 2018 Jan 17. Surg Endosc. 2018. PMID: 29344783 Free PMC article.
-
Management of pancreatic fluid collections: A comprehensive review of the literature.World J Gastroenterol. 2016 Feb 21;22(7):2256-70. doi: 10.3748/wjg.v22.i7.2256. World J Gastroenterol. 2016. PMID: 26900288 Free PMC article. Review.
Cited by
-
Single transluminal gateway transcystic multiple drainage for extensive walled-off pancreatic necrosis - a single-centre experience.Prz Gastroenterol. 2018;13(3):242-248. doi: 10.5114/pg.2018.78290. Epub 2018 Sep 17. Prz Gastroenterol. 2018. PMID: 30302171 Free PMC article.
-
Endotherapy for pancreatic necrosis: An update.JGH Open. 2018 Dec 7;3(1):80-88. doi: 10.1002/jgh3.12109. eCollection 2019 Feb. JGH Open. 2018. PMID: 30834345 Free PMC article. Review.
-
Disconnected pancreatic duct syndrome in patients with necrotizing pancreatitis.Surg Open Sci. 2022 Nov 11;11:19-25. doi: 10.1016/j.sopen.2022.10.009. eCollection 2023 Jan. Surg Open Sci. 2022. PMID: 36438587 Free PMC article.
-
Cost-effectiveness of benign Wirsung duct strictures treatment in chronic pancreatitis.Wideochir Inne Tech Maloinwazyjne. 2018 Mar;13(1):17-26. doi: 10.5114/wiitm.2018.72578. Epub 2018 Jan 4. Wideochir Inne Tech Maloinwazyjne. 2018. PMID: 29643954 Free PMC article.
-
Various Modalities Accurate in Diagnosing a Disrupted or Disconnected Pancreatic Duct in Acute Pancreatitis: A Systematic Review.Dig Dis Sci. 2021 May;66(5):1415-1424. doi: 10.1007/s10620-020-06413-0. Epub 2020 Jun 27. Dig Dis Sci. 2021. PMID: 32594462 Free PMC article.
References
-
- da Costa DW, Boerma D, van Santvoort HC, et al. Staged multidisciplinary step-up management for necrotizing pancreatitis. Br J Surg. 2014;101:e65–79. - PubMed
-
- Smoczyński M, Marek I, Dubowik M, et al. Endoscopic drainage/debridement of walled-off pancreatic necrosis – single center experience of 112 cases. Pancreatology. 2014;14:137–42. - PubMed
-
- Devière J, Antaki F. Disconnected pancreatic tail syndrome: a plea for multidisciplinarity. Gastrointest Endosc. 2008;67:680–2. - PubMed
-
- Varadarajulu S, Noone TC, Tutuian R, Hawes RH, Cotton PB. Predictors of outcome in pancreatic duct disruption managed by endoscopic transpapillary stent placement. Gastrointest Endosc. 2005;61:568–75. - PubMed
-
- Thoeni RF. The revised Atlanta classification of acute pancreatitis: its importance for the radiologist and its effect on treatment. Radiology. 2012;262:751–64. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources