

Magnetic Resonance Imaging after Completion of Neoadjuvant Chemotherapy Can Accurately Discriminate between No Residual Carcinoma and Residual Ductal Carcinoma In Situ in Patients with Triple-Negative Breast Cancer
- PMID: 26866475
- PMCID: PMC4750980
- DOI: 10.1371/journal.pone.0149347
Magnetic Resonance Imaging after Completion of Neoadjuvant Chemotherapy Can Accurately Discriminate between No Residual Carcinoma and Residual Ductal Carcinoma In Situ in Patients with Triple-Negative Breast Cancer
Abstract
Background: The accurate evaluation of favorable response to neoadjuvant chemotherapy (NCT) is critical to determine the extent of surgery. We investigated independent clinicopathological and radiological predictors to discriminate no residual carcinoma (ypT0) from residual ductal carcinoma in situ (ypTis) in breast cancer patients who received NCT.
Patients and methods: Parameters of 117 patients attaining pathological complete response (CR) in the breast after NCT between January 2010 and December 2013 were retrospectively evaluated by univariate and multivariate analyses. All patients underwent mammography, ultrasound, and magnetic resonance imaging (MRI) before and after NCT.
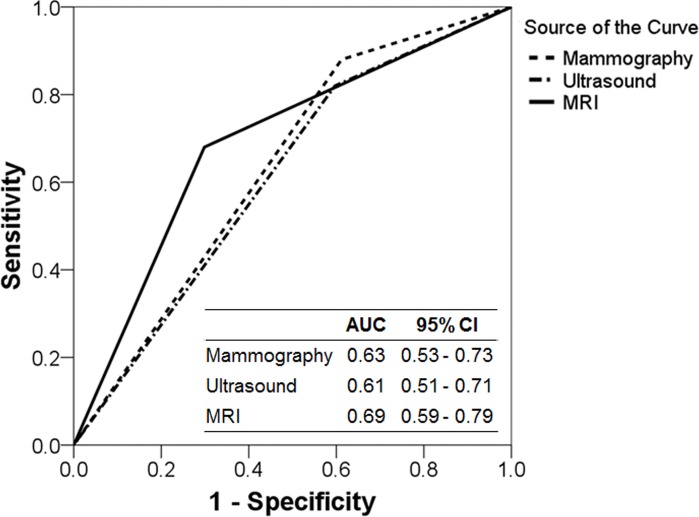
Results: There were 67 (57.3%) patients with ypT0. These patients were associated with hormone receptor-negative status, human epidermal growth factor receptor-2 (HER2)-negative tumors, and a higher likelihood of breast-conservation surgery. Baseline mammographic and MRI presentation of the main lesion, absence of associated microcalcifications, shape, posterior features, and absence of calcifications on ultrasound were significantly associated with ypT0. CR in mammography, ultrasound, or MRI after NCT was also related to ypT0. By multivariate analysis, independent predictors of ypT0 were the triple-negative subtype [Odds ratio (OR), 4.23; 95% confidence interval (CI), 1.11-16.09] and CR in MRI after NCT (OR, 5.23; 95% CI, 1.53-17.85). Stratified analysis by breast cancer subtype demonstrated that MRI well predicted ypT0 in all subtypes except the HER2-positive subtype. In particular, of 40 triple-negative subtypes, 22 showed CR in MRI and 21 (95.5%) were ypT0 after NCT.
Conclusion: Among imaging modalities, breast MRI can potentially distinguish between ypT0 and ypTis after NCT, especially in patients with triple-negative breast cancer. This information can help clinicians evaluate tumor response to NCT and plan surgery for breast cancer patients of all subtypes except for those with HER2-enriched tumors after NCT.
Conflict of interest statement
Figures
References
-
- Berruti A, Generali D, Kaufmann M, Puztai L, Curigliano G, Aglietta M, et al. International expert consensus on primary systemic therapy in the management of early breast cancer: highlights of the Fourth Symposium on Primary Systemic Therapy in the Management of Operable Breast Cancer, Cremona, Italy (2010). J Natl Cancer Inst Monogr. 2011;2011: 147–151. 10.1093/jncimonographs/lgr037 . - DOI - PubMed
-
- Kaufmann M, von Minckwitz G, Mamounas EP, Cameron D, Carey LA, Cristofanilli M, et al. Recommendations from an international consensus conference on the current status and future of neoadjuvant systemic therapy in primary breast cancer. Ann Surg Oncol. 2012;19: 1508–1516. 10.1245/s10434-011-2108-2 . - DOI - PubMed
-
- Chen K, Jia W, Li S, He J, Zeng Y, Yang H, et al. Cavity margin status is an independent risk factor for local-regional recurrence in breast cancer patients treated with neoadjuvant chemotherapy before breast-conserving surgery. Am Surg. 2011;77: 1700–1706. . - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
