

Epidemiology and Burden of Bloodstream Infections Caused by Extended-Spectrum Beta-Lactamase Producing Enterobacteriaceae in a Pediatric Hospital in Senegal
- PMID: 26867226
- PMCID: PMC4750952
- DOI: 10.1371/journal.pone.0143729
Epidemiology and Burden of Bloodstream Infections Caused by Extended-Spectrum Beta-Lactamase Producing Enterobacteriaceae in a Pediatric Hospital in Senegal
Abstract
Context: Severe bacterial infections are not considered as a leading cause of death in young children in sub-Saharan Africa. The worldwide emergence of extended-spectrum beta-lactamase producing Enterobacteriaceae (ESBL-E) could change the paradigm, especially in neonates who are at high risk of developing healthcare-associated infections.
Objective: To evaluate the epidemiology and the burden of ESBL-E bloodstream infections (BSI).
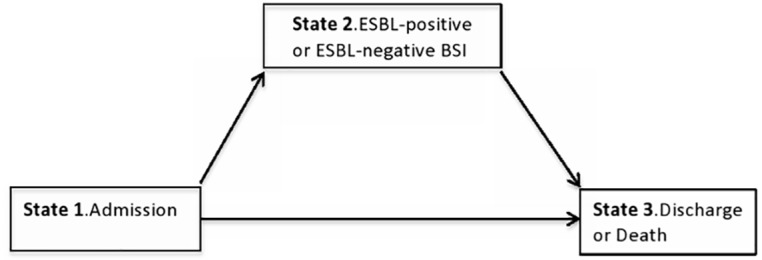
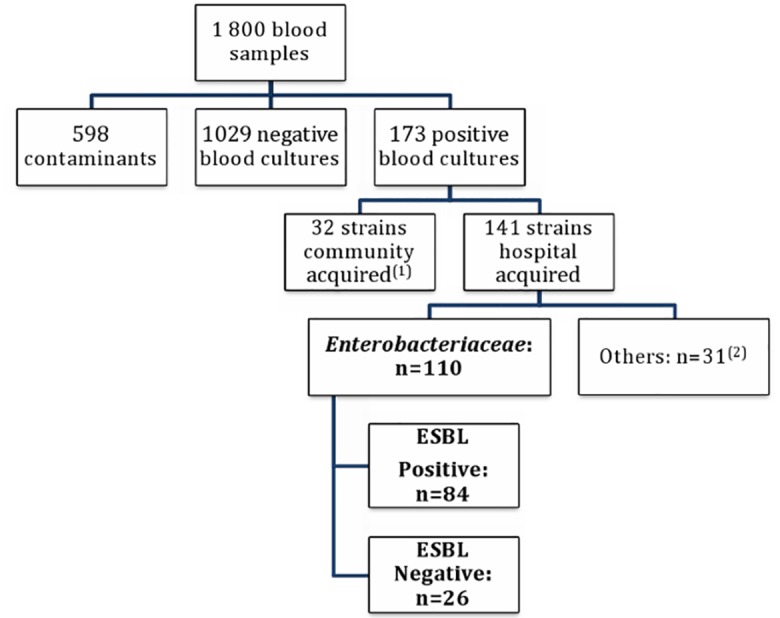
Methods: A case-case-control study was conducted in patients admitted in a pediatric hospital during two consecutive years. Cases were patients with Enterobacteriaceae BSI and included ESBL-positive (cases 1) and ESBL-negative BSI (cases 2). Controls were patients with no BSI. Multivariate analysis using a stepwise logistic regression was performed to identify risk factors for ESBL acquisition and for fatal outcomes. A multistate model was used to estimate the excess length of hospital stay (LOS) attributable to ESBL production while accounting for time of infection. Cox proportional hazards models were performed to assess the independent effect of ESBL-positive and negative BSI on LOS.
Results: The incidence rate of ESBL-E BSI was of 1.52 cases/1000 patient-days (95% CI: 1.2-5.6 cases per 1000 patient-days). Multivariate analysis showed that independent risk factors for ESBL-BSI acquisition were related to underlying comorbidities (sickle cell disease OR = 3.1 (95%CI: 2.3-4.9), malnutrition OR = 2.0 (95%CI: 1.7-2.6)) and invasive procedures (mechanical ventilation OR = 3.5 (95%CI: 2.7-5.3)). Neonates were also identified to be at risk for ESBL-E BSI. Inadequate initial antibiotic therapy was more frequent in ESBL-positive BSI than ESBL-negative BSI (94.2% versus 5.7%, p<0.0001). ESBL-positive BSI was associated with higher case-fatality rate than ESBL-negative BSI (54.8% versus 15.4%, p<0.001). Multistate modelling indicated an excess LOS attributable to ESBL production of 4.3 days. The adjusted end-of-LOS hazard ratio for ESBL-positive BSI was 0.07 (95%CI, 0.04-0.12).
Conclusion: Control of ESBL-E spread is an emergency in pediatric populations and could be achieved with simple cost-effective measures such as hand hygiene, proper management of excreta and better stewardship of antibiotic use, especially for empirical therapy.
Conflict of interest statement
Figures
References
-
- Bryce J, Boschi-Pinto C, Shibuya K, Black RE and the WHO Child Health Epidemiology Reference Group. WHO estimates of the causes of death in children. Lancet. 2005; 365:1147–1152. - PubMed
-
- Lawn JE, Cousens S, Zupan J. Four million neonatal deaths: When? Where? Why? Lancet. 2005; 365:891–900. - PubMed
-
- Seale AC, Blencowe H, Manu AA, Nair H, Bahl R, Qazi SA et al. Estimates of possible severe bacterial infection in neonates in sub-Saharan Africa, south Asia, and Latin America for 2012: a systematic review and meta-analysis. The Lancet Infectious Diseases. 2014; 14: 731–741 10.1016/S1473-3099(14)70804-7 - DOI - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
