

Skilled Bimanual Training Drives Motor Cortex Plasticity in Children With Unilateral Cerebral Palsy
- PMID: 26867559
- PMCID: PMC4981562
- DOI: 10.1177/1545968315625838
Skilled Bimanual Training Drives Motor Cortex Plasticity in Children With Unilateral Cerebral Palsy
Abstract
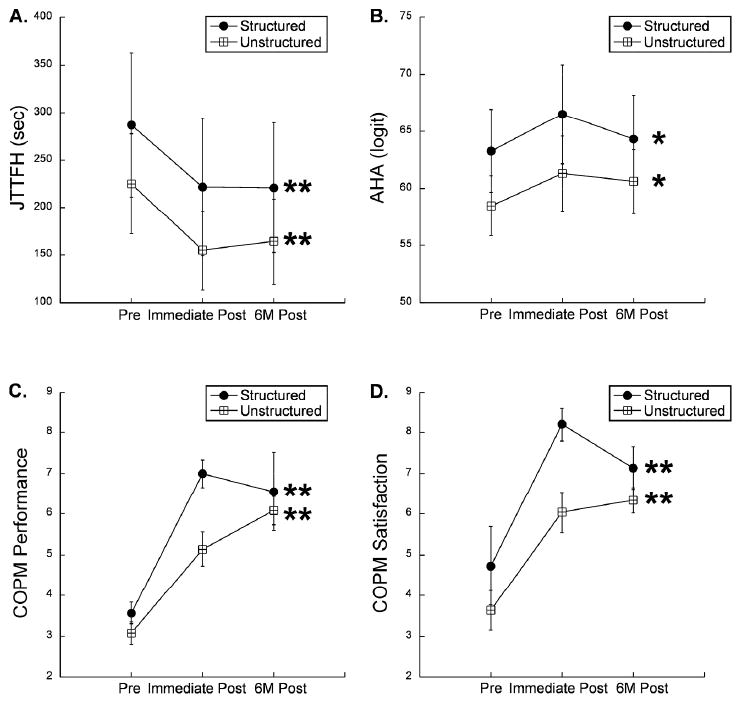
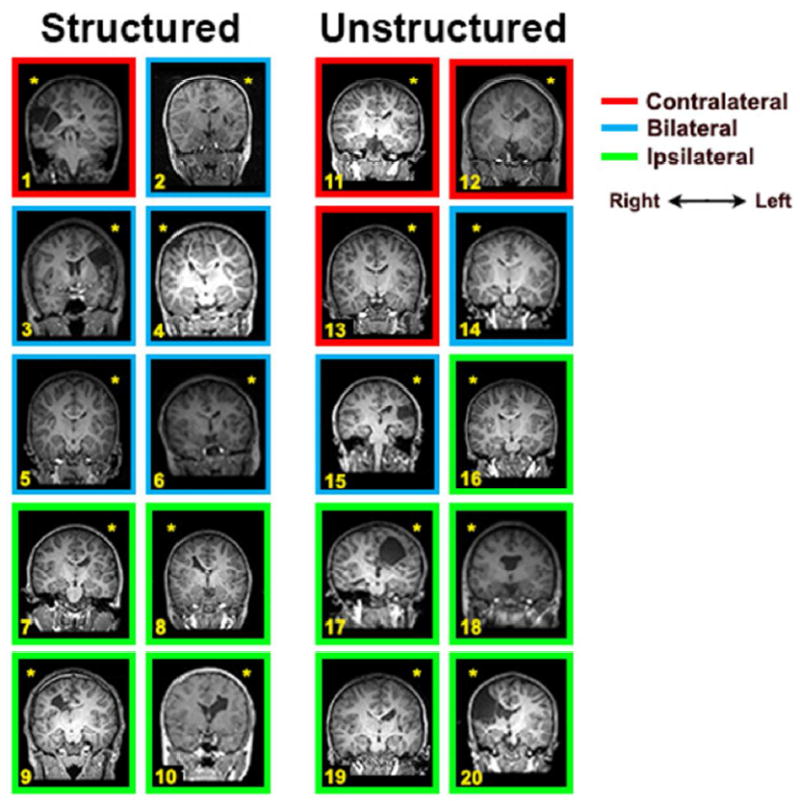
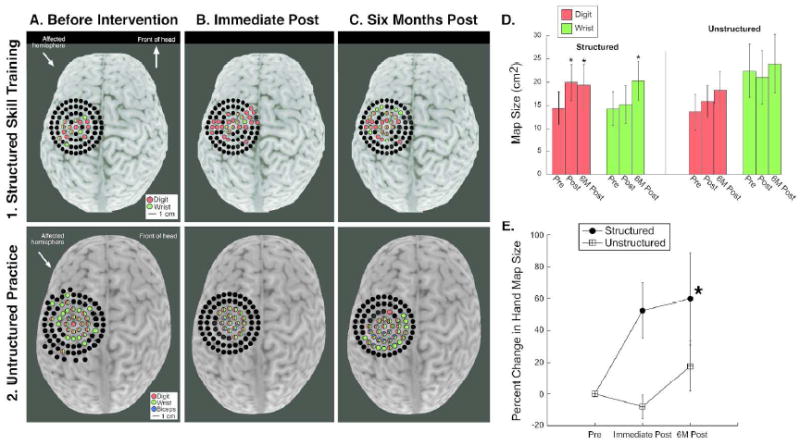
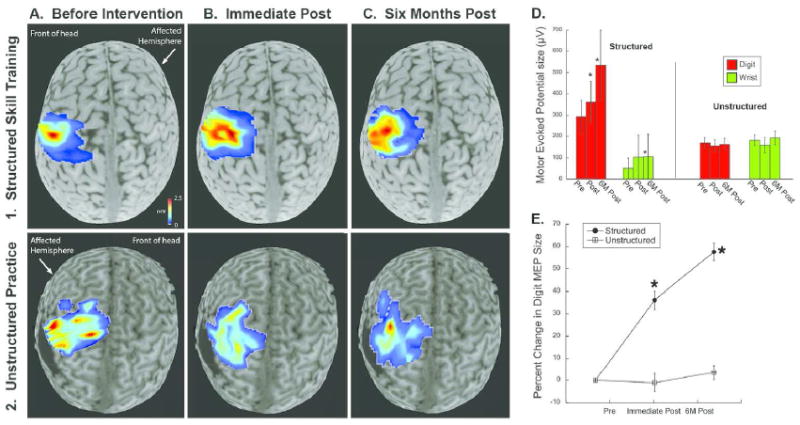
Background Intensive bimanual therapy can improve hand function in children with unilateral spastic cerebral palsy (USCP). We compared the effects of structured bimanual skill training versus unstructured bimanual practice on motor outcomes and motor map plasticity in children with USCP. Objective We hypothesized that structured skill training would produce greater motor map plasticity than unstructured practice. Methods Twenty children with USCP (average age 9.5; 12 males) received therapy in a day camp setting, 6 h/day, 5 days/week, for 3 weeks. In structured skill training (n = 10), children performed progressively more difficult movements and practiced functional goals. In unstructured practice (n = 10), children engaged in bimanual activities but did not practice skillful movements or functional goals. We used the Assisting Hand Assessment (AHA), Jebsen-Taylor Test of Hand Function (JTTHF), and Canadian Occupational Performance Measure (COPM) to measure hand function. We used single-pulse transcranial magnetic stimulation to map the representation of first dorsal interosseous and flexor carpi radialis muscles bilaterally. Results Both groups showed significant improvements in bimanual hand use (AHA; P < .05) and hand dexterity (JTTHF; P < .001). However, only the structured skill group showed increases in the size of the affected hand motor map and amplitudes of motor evoked potentials (P < .01). Most children who showed the most functional improvements (COPM) had the largest changes in map size. Conclusions These findings uncover a dichotomy of plasticity: the unstructured practice group improved hand function but did not show changes in motor maps. Skill training is important for driving motor cortex plasticity in children with USCP.
Keywords: hemiplegia; neuroplasticity; pediatric; rehabilitation; transcranial magnetic stimulation.
© The Author(s) 2016.
Figures
Comment in
-
Commentary: Skilled Bimanual Training Drives Motor Cortex Plasticity in Children With Unilateral Cerebral Palsy.Front Hum Neurosci. 2017 Jun 7;11:297. doi: 10.3389/fnhum.2017.00297. eCollection 2017. Front Hum Neurosci. 2017. PMID: 28638332 Free PMC article. No abstract available.
References
-
- Gordon AM, Chinnan A, Gill S, Petra E, Hung YC, Charles J. Both constraint-induced movement therapy and bimanual training lead to improved performance of upper extremity function in children with hemiplegia. Developmental medicine and child neurology. 2008 Dec;50(12):957–958. - PubMed
-
- Gordon AM, Hung YC, Brandao M, et al. Bimanual training and constraint-induced movement therapy in children with hemiplegic cerebral palsy: a randomized trial. Neurorehabilitation and neural repair. 2011 Oct;25(8):692–702. - PubMed
-
- Gordon AM, Schneider JA, Chinnan A, Charles JR. Efficacy of a hand-arm bimanual intensive therapy (HABIT) in children with hemiplegic cerebral palsy: a randomized control trial. Developmental medicine and child neurology. 2007 Nov;49(11):830–838. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
