

Status quo and directions in deep head and neck hyperthermia
- PMID: 26868027
- PMCID: PMC4751675
- DOI: 10.1186/s13014-016-0588-8
Status quo and directions in deep head and neck hyperthermia
Abstract
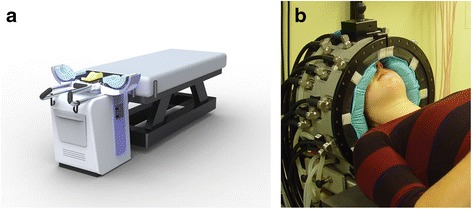
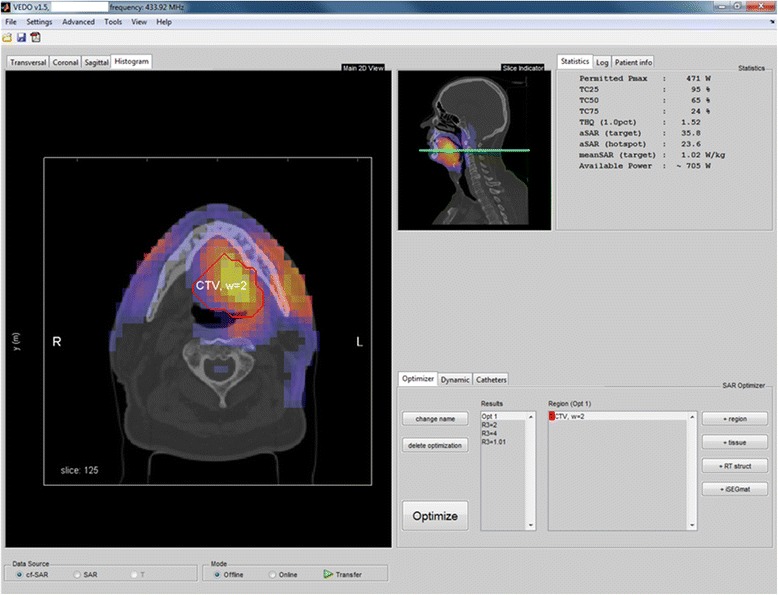
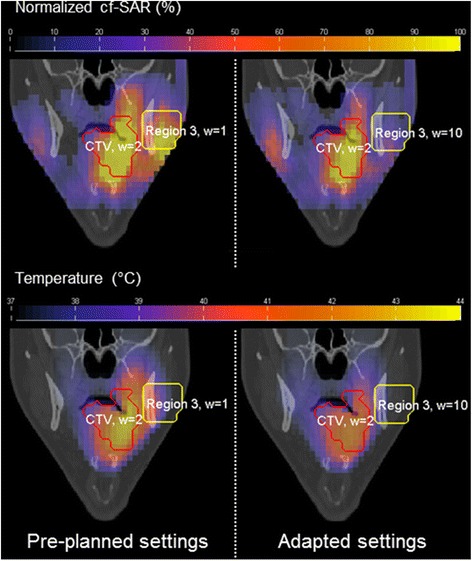
The benefit of hyperthermia as a potent modifier of radiotherapy has been well established and more recently also the combination with chemotherapy was shown beneficial. Also for head and neck cancer, the impact of hyperthermia has been clinically demonstrated by a number of clinical trials. Unfortunately, the technology applied in these studies provided only limited thermal dose control, and the devices used only allowed treatment of target regions close to the skin. Over the last decade, we developed the technology for deep and controlled hyperthermia that allows treatment of the entire head and neck region. Our strategy involves focused microwave heating combined with 3D patient-specific electromagnetic and thermal simulations for conformal, reproducible and adaptive hyperthermia application. Validation of our strategy has been performed by 3D thermal dose assessment based on invasively placed temperature sensors combined with the 3D patient specific simulations. In this paper, we review the phase III clinical evidence for hyperthermia in head and neck tumors, as well as the heating and dosimetry technology applied in these studies. Next, we describe the development, clinical implementation and validation of 3D guided deep hyperthermia with the HYPERcollar, and its second generation, i.e. the HYPERcollar3D. Lastly, we discuss early clinical results and provide an outlook for this technology.
Figures

References
-
- Nutting CM, Morden JP, Harrington KJ, Urbano TG, Bhide SA, Clark C, et al. Parotid-sparing intensity modulated versus conventional radiotherapy in head and neck cancer (PARSPORT): a phase 3 multicentre randomised controlled trial. Lancet Oncol. 2011;12(2):127–36. doi: 10.1016/S1470-2045(10)70290-4. - DOI - PMC - PubMed
-
- Ling TC, Slater JM, Nookala P, Mifflin R, Grove R, Ly AM, et al. Analysis of Intensity-Modulated Radiation Therapy (IMRT), Proton and 3D Conformal Radiotherapy (3D-CRT) for Reducing Perioperative Cardiopulmonary Complications in Esophageal Cancer Patients. Cancers (Basel) 2014;6(4):2356–68. doi: 10.3390/cancers6042356. - DOI - PMC - PubMed
-
- Pignon JP, Bourhis J, Domenge C, Designe L. Chemotherapy added to locoregional treatment for head and neck squamous-cell carcinoma: three meta-analyses of updated individual data. MACH-NC Collaborative Group. Meta-Analysis of Chemotherapy on Head and Neck Cancer. Lancet. 2000;355(9208):949–55. doi: 10.1016/S0140-6736(00)90011-4. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
