

Extended Self-Help for Smoking Cessation: A Randomized Controlled Trial
- PMID: 26868284
- PMCID: PMC4914420
- DOI: 10.1016/j.amepre.2015.12.016
Extended Self-Help for Smoking Cessation: A Randomized Controlled Trial
Abstract
Introduction: Far too few smokers receive recommended interventions at their healthcare visits, highlighting the importance of identifying effective, low-cost smoking interventions that can be readily delivered. Self-help interventions (e.g., written materials) would meet this need, but they have shown low efficacy. The purpose of this RCT was to determine the efficacy of a self-help intervention with increased duration and intensity.
Design: Randomized parallel trial design involving enrollment between April 2010 and August 2011 with follow-up data for 24 months.
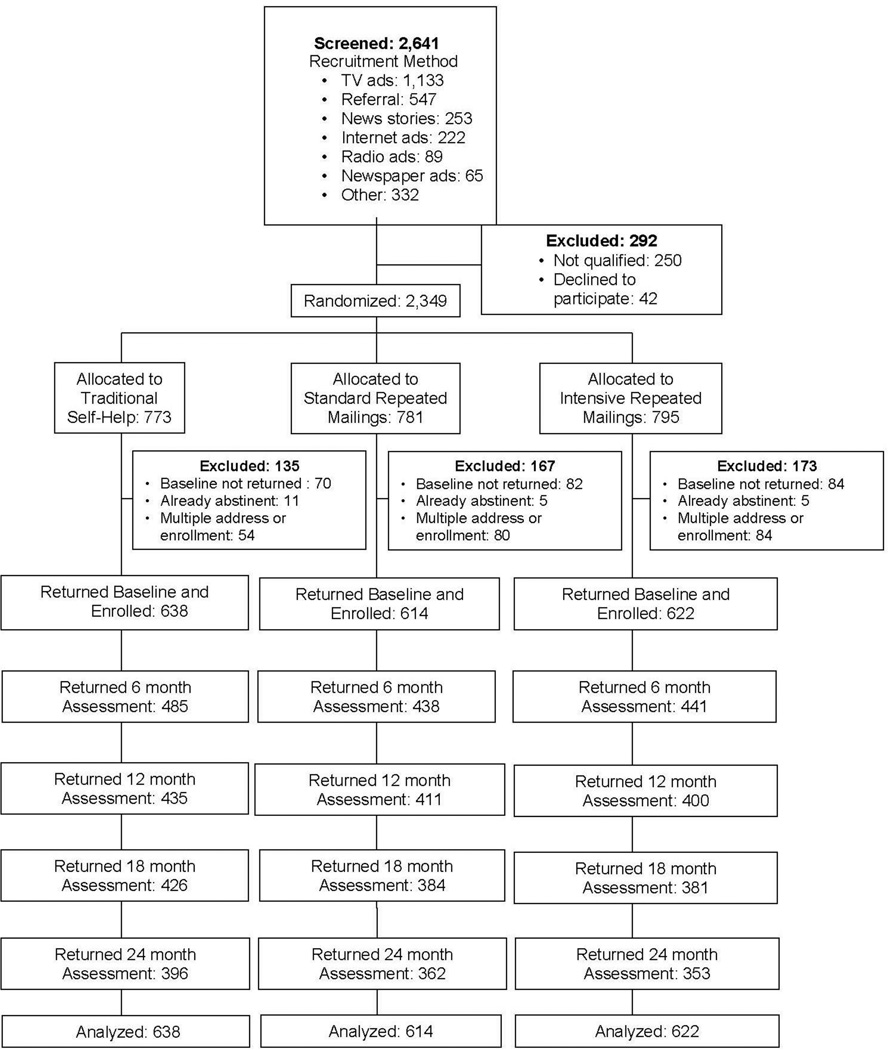
Setting/participants: U.S. national sample of daily smokers (N=1,874).
Intervention: Participants were randomized to one of three arms of a parallel trial design: Traditional Self-Help (TSH, n=638), Standard Repeated Mailings (SRM, n=614), or Intensive Repeated Mailings (IRM, n=622). TSH received an existing self-help booklet for quitting smoking. SRM received eight different cessation booklets mailed over a 12-month period. IRM received monthly mailings of ten booklets and additional material designed to enhance social support over 18 months.
Main outcome measures: The primary outcome was 7-day point-prevalence abstinence collected at 6, 12, 18, and 24 months.
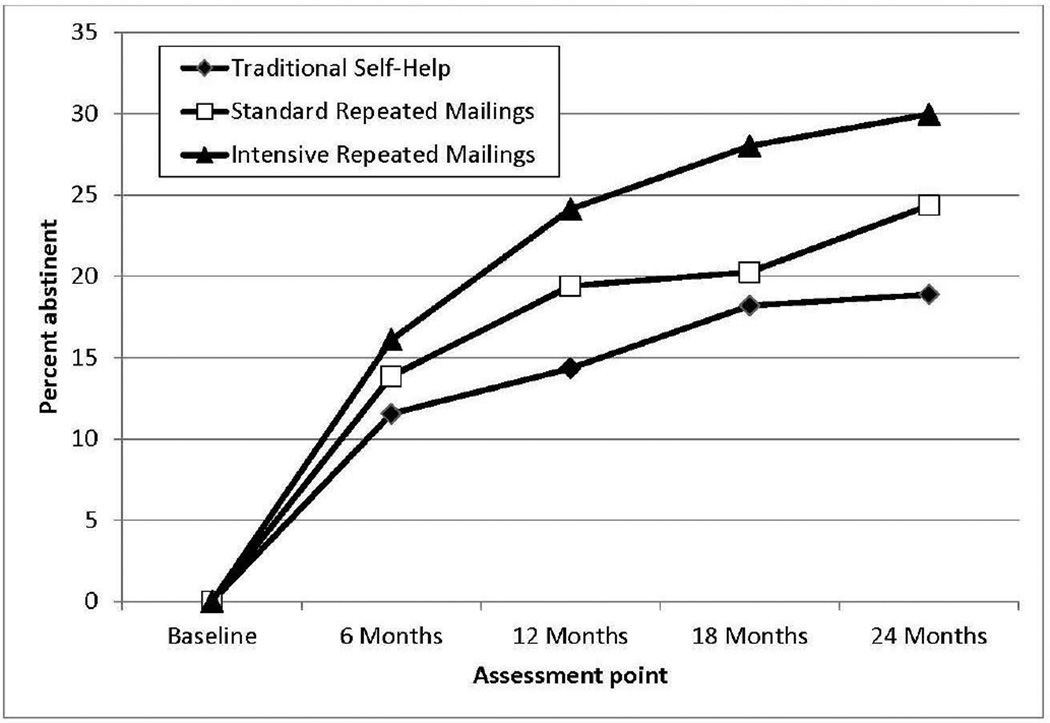
Results: Data were analyzed between 2013 and 2015. A dose-response effect was found across all four follow-up points. For example, by 24 months, IRM produced the highest abstinence rate (30.0%), followed by SRM (24.4%) and TSH (18.9%). The difference in 24-month abstinence rates between IRM and TSH was 11.0% (95% CI=5.7%, 16.3%). Cost analyses indicated that, compared with TSH, the incremental cost per quitter who received SRM and IRM was $560 and $361, respectively.
Conclusions: Self-help interventions with increased intensity and duration resulted in significantly improved abstinence rates that extended 6 months beyond the end of the intervention. Despite the greater intensity, the interventions were highly cost effective, suggesting that widespread dissemination in healthcare settings could greatly enhance quitting.
Trial registration: This study is registered at www.clinicaltrials.gov NCT01352195.
Copyright © 2016 American Journal of Preventive Medicine. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Jha P, Peto R. Global Health: Global Effects of Smoking, of Quitting, and of Taxing Tobacco. N Engl J Med. 2014;370(1):60–68. http://dx.doi.org/10.1056/NEJMra1308383. - DOI - PubMed
-
- Pierce JP, Cummins SE, White MM, Humphrey A, Messer K. Quitlines and nicotine replacement for smoking cessation: Do we need to change policy? Annu Rev Public Health. 2012;33:341–356. http://dx.doi.org/10.1146/annurev-publhealth-031811-124624. - DOI - PubMed
-
- Papadakis S, McDonald P, Mullen KA, Reid R, Skulsky K, Pipe A. Strategies to increase the delivery of smoking cessation treatments in primary care settings: A systematic review and meta-analysis. Prev Med. 2010;51(3–4):199–213. http://dx.doi.org/10.1016/j.ypmed.2010.06.007. - DOI - PubMed
-
- Hartmann-Boyce J, Lancaster T, Stead L. Print-based self-help interventions for smoking cessation. Cochrane Database Syst Rev. 2014;6:CD001118. http://dx.doi.org/10.1002/14651858.cd001118.pub3. - DOI - PubMed
-
- Fiore MC, Jaen CR, Baker TB, et al. Treating tobacco use and dependence: 2008 update. Rockville, MD: U.S. DHHS, Public Health Service; 2008.
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
