

No Difference in Average Interdialytic Weight Gain Observed in a Randomized Trial With a Technology-Supported Behavioral Intervention to Reduce Dietary Sodium Intake in Adults Undergoing Maintenance Hemodialysis in the United States: Primary Outcomes of the BalanceWise Study
- PMID: 26868602
- PMCID: PMC5031139
- DOI: 10.1053/j.jrn.2015.11.006
No Difference in Average Interdialytic Weight Gain Observed in a Randomized Trial With a Technology-Supported Behavioral Intervention to Reduce Dietary Sodium Intake in Adults Undergoing Maintenance Hemodialysis in the United States: Primary Outcomes of the BalanceWise Study
Abstract
Objective: To evaluate the efficacy of behavioral counseling combined with technology-based self-monitoring for sodium restriction in hemodialysis (HD) patients.
Design: Randomized clinical trial.
Subjects: English literate adults undergoing outpatient, in-center intermittent HD for at least 3 months.
Interventions: Over a 16-week period, both the intervention and the attention control groups were shown 6 educational modules on the HD diet. The intervention group also received social cognitive theory-based behavioral counseling and monitored their diets daily using handheld computers.
Main outcome measures: Average daily interdialytic weight gain (IDWGA) was calculated for every week of HD treatment over the observation period by subtracting the post-dialysis weight at the previous treatment time (t-1) from the pre-dialysis weight at the current treatment time (t), dividing by the number of days between treatments. Three 24-hour dietary recalls were obtained at baseline, 8 weeks, and 16 weeks and evaluated using the Nutrient Data System for Research.
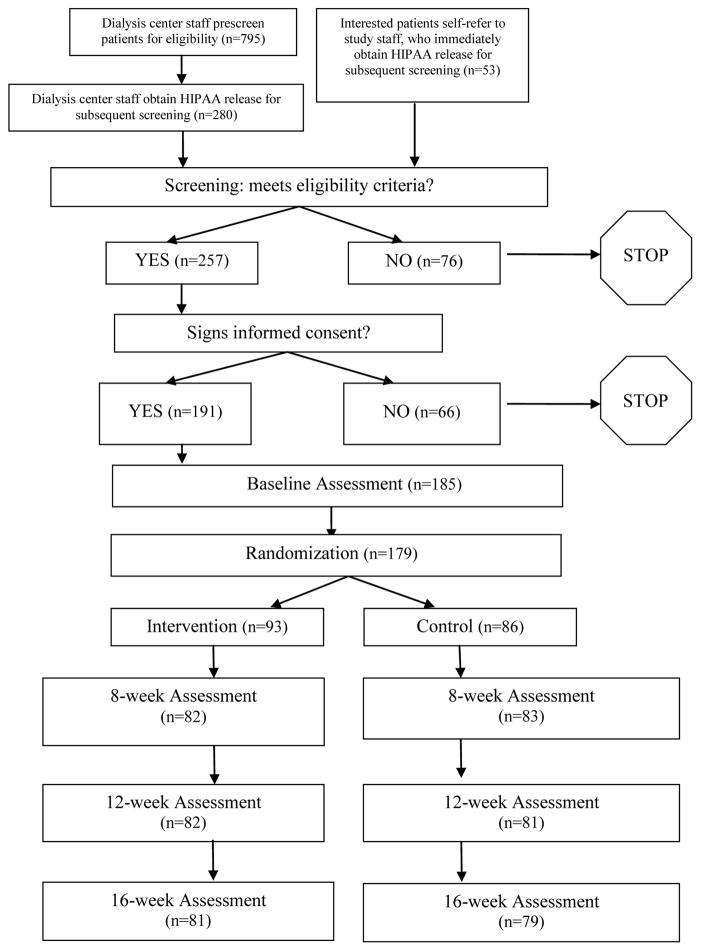
Results: A total of 179 participants were randomized, and 160 (89.4%) completed final measurements. IDWGA did not differ significantly by treatment group at any time point considered (P > .79 for each). A significant differential change in dietary sodium intake observed at 8 weeks (-372 mg/day; P = .05) was not sustained at 16 weeks (-191 mg/day; P = .32).
Conclusion: The BalanceWise Study intervention appeared to be feasible and acceptable to HD patients although IDWGA was unchanged and the desired behavioral changes observed at 8 weeks were not sustained. Unmeasured factors may have contributed to the mixed findings, and further research is needed to identify the appropriate patients for such interventions.
Trial registration: ClinicalTrials.gov NCT01125202.
Copyright © 2016 National Kidney Foundation, Inc. All rights reserved.
Figures
References
-
- USRDS. Annual Data Report. Volume 2: Atlas ESRD, Chapter 4 – Cardiovascular Disease. [Accessed March 26, 2015];2013 Available at: http://www.usrds.org/
-
- Rahman M, Dixit A, Donley V, et al. Factors associated with inadequate blood pressure control 8in hypertensive hemodialysis patients. Am J Clin Nutri. 1999;33(3):498–506. - PubMed
-
- Foley RN, Parfrey PS, Harnett JD, Kent GM, Murray DC, Barre PE. Impact of hypertension on cardiomyopathy, morbidity and mortality in end-stage renal disease. Kidney Int. 1996;49(5):1379–1385. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
