

Association of Compliance With Process-Related Quality Metrics and Improved Survival in Oral Cavity Squamous Cell Carcinoma
- PMID: 26869135
- PMCID: PMC6086583
- DOI: 10.1001/jamaoto.2015.3595
Association of Compliance With Process-Related Quality Metrics and Improved Survival in Oral Cavity Squamous Cell Carcinoma
Abstract
Importance: Quality metrics for patients with head and neck cancer are available, but it is unknown whether compliance with these metrics is associated with improved patient survival.
Objective: To identify whether compliance with various process-related quality metrics is associated with improved survival in patients with oral cavity squamous cell carcinoma who receive definitive surgery with or without adjuvant therapy.
Design, setting, and participants: A retrospective cohort study was conducted at a tertiary academic medical center among 192 patients with previously untreated oral cavity squamous cell carcinoma who underwent definitive surgery with or without adjuvant therapy between January 1, 2003, and December 31, 2010. Data analysis was performed from January 26 to August 7, 2015.
Interventions: Surgery with or without adjuvant therapy.
Main outcomes and measures: Compliance with a collection of process-related quality metrics possessing face validity that covered pretreatment evaluation, treatment, and posttreatment surveillance was evaluated. Association between compliance with these quality metrics and overall survival, disease-specific survival, and disease-free survival was calculated using univariable and multivariable Cox proportional hazards analysis.
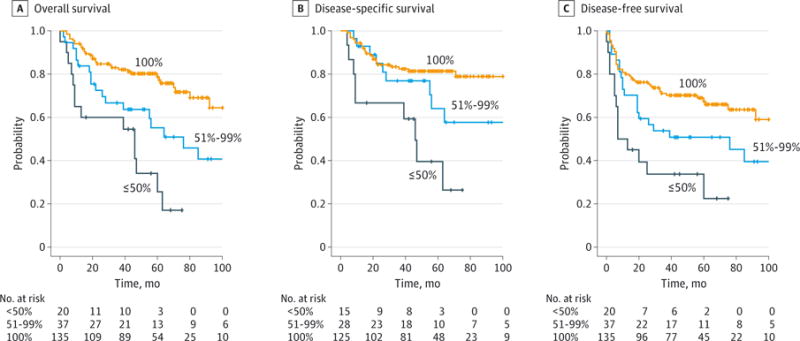
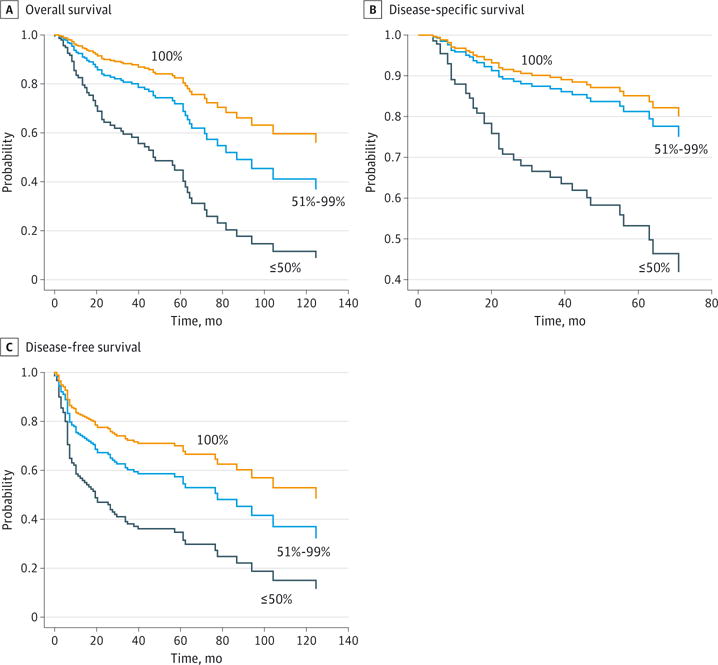
Results: Among 192 patients, compliance with the individual quality metrics ranged from 19.7% to 93.6% (median, 82.8%). No pretreatment or surveillance metrics were associated with improved survival. Compliance with the following treatment-related quality metrics was associated with improved survival: elective neck dissection with lymph node yield of 18 or more, no unplanned surgery within 14 days of the index surgery, no unplanned 30-day readmissions, and referral for adjuvant radiotherapy for pathologic stage III or IV disease. Increased compliance with a "clinical care signature" composed of these 4 metrics was associated with improved overall survival, disease-specific survival, and disease-free survival on univariable analysis (log-rank test; P < .05 for each). On multivariable analysis controlling for pT stage, pN stage, extracapsular spread, margin status, and comorbidity, increased compliance with these 4 metrics was associated with improved overall survival (100% vs ≤50% compliance: adjusted hazard ratio [aHR], 4.2; 95% CI, 2.1-8.5; 100% vs 51%-99% compliance: aHR, 1.7; 95% CI, 1.0-3.1), improved disease-specific survival (100% vs ≤50% compliance: aHR, 3.9; 95% CI, 1.7-9.0; 100% vs 51%-99%: aHR, 1.3; 95% CI, 0.6-2.9), and improved disease-free survival (100% vs ≤50% compliance: aHR, 3.0; 95% CI, 1.5-5.8; 100% vs 51%-99% compliance: aHR, 1.6; 95% CI, 0.9-2.7).
Conclusions and relevance: Compliance with a core set of process-related quality metrics was associated with improved survival for patients with surgically managed oral cavity squamous cell carcinoma. Multi-institutional validation of these metrics is warranted.
Conflict of interest statement
Conflict of Interest Disclosures: None reported.
Figures
Similar articles
-
Evaluation of Quality Metrics for Surgically Treated Laryngeal Squamous Cell Carcinoma.JAMA Otolaryngol Head Neck Surg. 2016 Dec 1;142(12):1154-1163. doi: 10.1001/jamaoto.2016.0657. JAMA Otolaryngol Head Neck Surg. 2016. PMID: 27435696 Free PMC article.
-
Analysis of Process-Related Quality Metrics and Survival of Patients with Oral Cavity Squamous Cell Carcinoma.Otolaryngol Head Neck Surg. 2019 Sep;161(3):450-457. doi: 10.1177/0194599819845864. Epub 2019 May 7. Otolaryngol Head Neck Surg. 2019. PMID: 31060452
-
Treatment Factors Associated With Survival in Early-Stage Oral Cavity Cancer: Analysis of 6830 Cases From the National Cancer Data Base.JAMA Otolaryngol Head Neck Surg. 2015 Jul;141(7):593-8. doi: 10.1001/jamaoto.2015.0719. JAMA Otolaryngol Head Neck Surg. 2015. PMID: 25974757
-
The impact of microscopic versus macroscopic extranodal extension in oral cavity squamous cell carcinoma: National cancer database analysis and review of the literature.Am J Otolaryngol. 2022 Jul-Aug;43(4):103511. doi: 10.1016/j.amjoto.2022.103511. Epub 2022 May 20. Am J Otolaryngol. 2022. PMID: 35609426 Review.
-
Survival of Young Versus Old Patients With Oral Cavity Squamous Cell Carcinoma: A Meta-Analysis.Laryngoscope. 2021 Jun;131(6):1310-1319. doi: 10.1002/lary.29260. Epub 2020 Dec 2. Laryngoscope. 2021. PMID: 33264444 Free PMC article.
Cited by
-
Treatment Patterns in Veterans with Laryngeal and Oropharyngeal Cancer and Impact on Survival.Laryngoscope Investig Otolaryngol. 2018 Aug 9;3(4):275-282. doi: 10.1002/lio2.170. eCollection 2018 Aug. Laryngoscope Investig Otolaryngol. 2018. PMID: 30186958 Free PMC article.
-
Effect of time to initiation of postoperative radiation therapy on survival in surgically managed head and neck cancer.Cancer. 2017 Dec 15;123(24):4841-4850. doi: 10.1002/cncr.30939. Epub 2017 Aug 25. Cancer. 2017. PMID: 28841234 Free PMC article.
-
Development and Evaluation of a Navigation-Based, Multilevel Intervention to Improve the Delivery of Timely, Guideline-Adherent Adjuvant Therapy for Patients With Head and Neck Cancer.JCO Oncol Pract. 2021 Oct;17(10):e1512-e1523. doi: 10.1200/OP.20.00943. Epub 2021 Mar 10. JCO Oncol Pract. 2021. PMID: 33689399 Free PMC article.
-
Best Practice in Surgical Treatment of Malignant Head and Neck Tumors.Front Oncol. 2020 Feb 12;10:140. doi: 10.3389/fonc.2020.00140. eCollection 2020. Front Oncol. 2020. PMID: 32117778 Free PMC article.
-
The Synthetic Flavonoid Derivative GL-V9 Induces Apoptosis and Autophagy in Cutaneous Squamous Cell Carcinoma via Suppressing AKT-Regulated HK2 and mTOR Signals.Molecules. 2020 Oct 30;25(21):5033. doi: 10.3390/molecules25215033. Molecules. 2020. PMID: 33143000 Free PMC article.
References
-
- Agency for Healthcare Research and Quality, US Dept of Health and Human Services. Your guide to choosing quality health care. http://archive.ahrq.gov/consumer/qnt/. Accessed May 30, 2015.
-
- McGlynn EA, Schneider EC, Kerr EA. Reimagining quality measurement. N Engl J Med. 2014;371(23):2150–2153. - PubMed
-
- Cassel CK, Conway PH, Delbanco SF, Jha AK, Saunders RS, Lee TH. Getting more performance from performance measurement. N Engl J Med. 2014;371(23):2145–2147. - PubMed
-
- Gourin CG, Couch ME. Defining quality in the era of health care reform. JAMA Otolaryngol Head Neck Surg. 2014;140(11):997–998. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
