

Surgical Repair of Abdominal Aortic and Renal Artery Aneurysms in Takayasu's Arteritis
- PMID: 26870600
- PMCID: PMC4733819
Surgical Repair of Abdominal Aortic and Renal Artery Aneurysms in Takayasu's Arteritis
Abstract
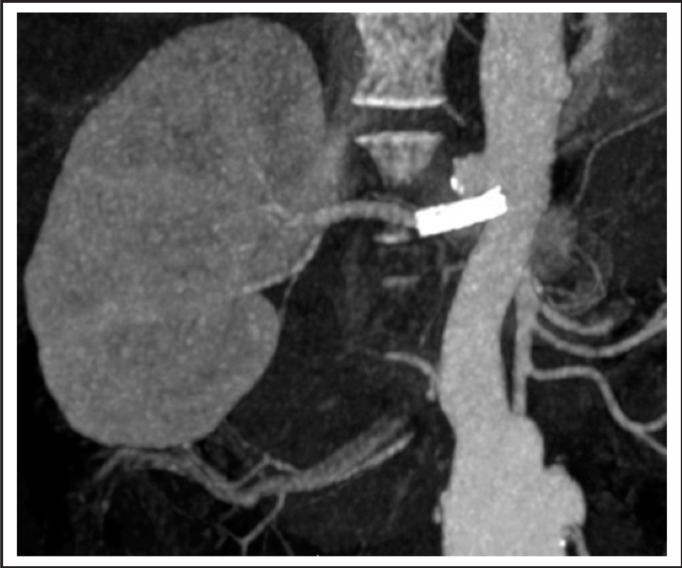
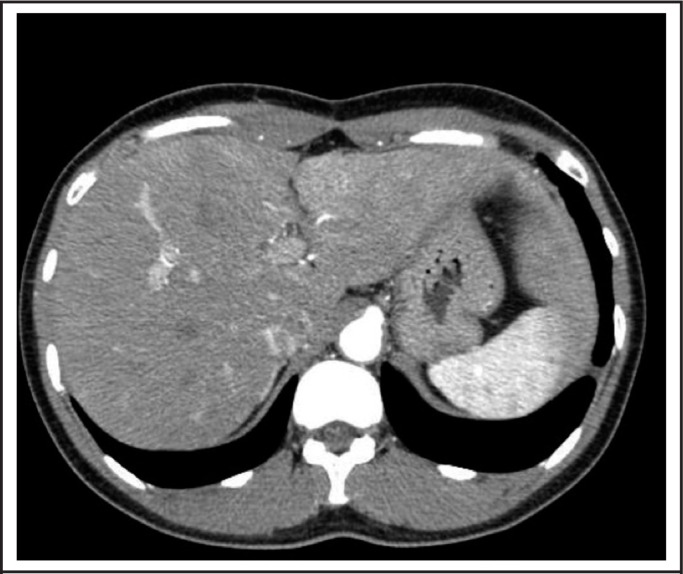
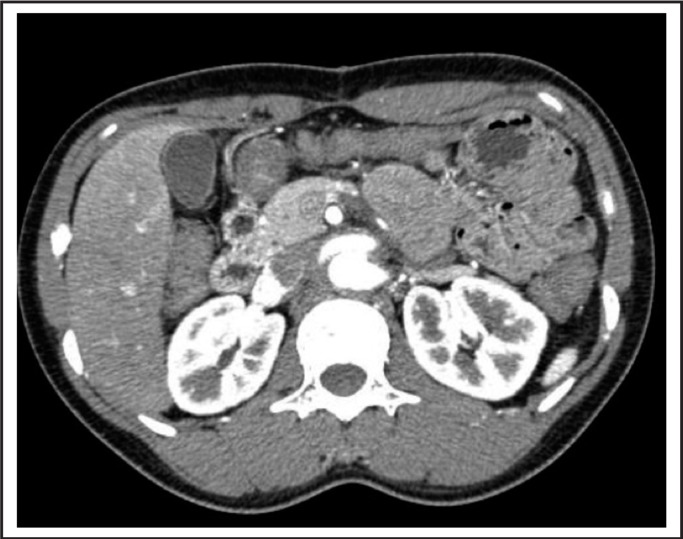
Takayasu's arteritis is a large vessel vasculitis that can be a challenging diagnosis to make and has a varied clinical presentation. Management largely depends on affected vessel disease severity and individual patient considerations. The diagnosis must be considered in a young patient with large vessel aneurysms. We present a case of a 30 year-old woman of Pacific Islander descent who presented to the Tripler Army medical Center Vascular Surgery Department in Honolulu, Hawai'i seeking repair of her abdominal aortic and renal artery aneurysms prior to conception. A 30 year-old Pacific Islander woman with a history of a saccular abdominal aortic aneurysm and renal artery aneurysms presented to our clinic seeking vascular surgery consultation prior to a planned pregnancy. She had a renal artery stent placed at an outside institution for hypertension. She met the diagnosis of Takayasu's arteritis by Sharma's criteria. Physical exam was significant for a palpable, pulsatile, abdominal mass and CT angiography revealed a saccular irregular-appearing infra-renal abdominal aortic aneurysm, extending to the aortic bifurcation, with a maximum diameter of 3.3 cm. A right renal artery aneurysm was also identified proximally, contiguous with the aorta, with a maximal transverse diameter of 1.7 cm. The patient underwent a supraceliac bypass to the right renal artery with a 7 mm Dacron graft, as well as excision of the right renal artery aneurysm. The abdominal aortic aneurysm was replaced using a Hemashield Dacron bifurcated 14 mm x 7 mm bypass graft. Intraoperative measurements of the renal artery aneurysm were 1.5 x 1.5 cm and the saccular appearing distal abdominal aortic aneurysm measured 3.6 x 3.3 cm. The patient was discharged from the hospital 7 days post-operatively. At 1-year follow up, CT scan of the abdominal aorta revealed the repair was without any evidence of aneurysm formation, anastomotic pseudoaneurysm formation, or areas of stenosis. She has remained normotensive with a normal serum creatinine 18 months after her repair. She has since delivered her second child. It is rare for Takayasu's arteritis to present with aneurysmal disease. It is much more common to present with stenosis or occlusion. It has yet to be proven that Takayasu's truly has a higher incidence in those of Asian descent. Takayasu's can be a difficult diagnosis to make but can be aided with the use of Sharma's criteria. Our particular patient posed unique considerations on the effects of the physiology of pregnancy on her aneurysms and repair. Managing the active phases of disease is imperative, and though medical management is first line, surgical intervention may be necessary. Surgical intervention should be performed in a quiescent period of disease if possible given that biological inflammation at the time of intervention increases the complication rate. Repair of aneurysmal disease in a young female should also be considered prior to pregnancy.
Keywords: Abdominal Aortic Aneurysm; Arterial Aneurysms; Pregnancy; Renal Artery Aneurysm.
Figures

Similar articles
-
[Surgery of abdominal aorta with horseshoe kidney].Srp Arh Celok Lek. 1997 Jan-Feb;125(1-2):36-44. Srp Arh Celok Lek. 1997. PMID: 17974353 Serbian.
-
Descending thoracic and thoracoabdominal aortic aneurysm in patients with Takayasu's disease.Ann Vasc Surg. 2004 Sep;18(5):505-13. doi: 10.1007/s10016-004-0073-y. Epub 2004 Aug 6. Ann Vasc Surg. 2004. PMID: 15534728
-
Subclavian artery aneurysm: an unusual manifestation of Takayasu's arteritis.Cardiovasc Surg. 1999 Apr;7(3):310-4. doi: 10.1016/s0967-2109(98)00171-9. Cardiovasc Surg. 1999. PMID: 10386748
-
Surgical treatment of Takayasu's arteritis: case report and literature review.Ann Vasc Surg. 2000 Mar;14(2):125-9. doi: 10.1007/s100169910023. Ann Vasc Surg. 2000. PMID: 10742426 Review.
-
[Surgical treatment of intractable vasculitis syndromes--with special reference to Buerger disease, Takayasu arteritis, and so-called inflammatory abdominal aortic aneurysm].Nihon Rinsho. 1994 Aug;52(8):2192-202. Nihon Rinsho. 1994. PMID: 7933611 Review. Japanese.
Cited by
-
Ex vivo revascularization of renal artery aneurysms in a patient with solitary kidney: A case report.World J Clin Cases. 2019 Aug 26;7(16):2401-2405. doi: 10.12998/wjcc.v7.i16.2401. World J Clin Cases. 2019. PMID: 31531337 Free PMC article.
-
Exceptional multisite aneurysms in Takayasu arteritis: A unique and challenging case.Radiol Case Rep. 2024 May 22;19(8):3345-3348. doi: 10.1016/j.radcr.2024.04.056. eCollection 2024 Aug. Radiol Case Rep. 2024. PMID: 38832341 Free PMC article.
References
-
- Stanley JC, Veith FJ, Wakefield TW. Current therapy in vascular and endovascular surgery. 5th edition. ed. Philadelphia, PA: Elsevier/Saunders; 2014.
-
- Sharma BK, Jain S, Suri S, Numano F. Diagnostic criteria for Takayasu arteritis. International Journal of Cardiology. 1996 Aug;54(Suppl):S141–S147. - PubMed
-
- Kallappa Parameshwarapp S, Mandjiny N, Kavumkal Rajagopalan B, Radhakrishnan N, Samavedam S, Unnikrishnan M. Intact giant abdominal aortic aneurysm due to Takayasu arteritis. Annals of Vascular Surgery. 2013 Jul;27(5):671. e611–674. - PubMed
-
- Lakhi NA, Jones J. Takayasu's arteritis in pregnancy complicated by peripartum aortic dissection. Archives of Gynecology and Obstetrics. 2010 Jul;282(1):103–106. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous