

Immunolocalization and Distribution of Rubella Antigen in Fatal Congenital Rubella Syndrome
- PMID: 26870820
- PMCID: PMC4739417
- DOI: 10.1016/j.ebiom.2015.11.050
Immunolocalization and Distribution of Rubella Antigen in Fatal Congenital Rubella Syndrome
Abstract
Background: An estimated 100,000 cases of congenital rubella syndrome (CRS) occur worldwide each year. The reported mortality rate for infants with CRS is up to 33%. The cellular mechanisms responsible for the multiple congenital defects in CRS are presently unknown. Here we identify cell types positive for rubella virus (RV) in CRS infants.
Methods: Cells and organs involved in RV replication were identified in paraffin-embedded autopsy tissues from three fatal case-patients by histopathologic examination and immunohistochemical (IHC) staining using a rabbit polyclonal RV antibody. Normal rabbit antisera and RV antisera preabsorbed with highly purified RV served as negative controls.
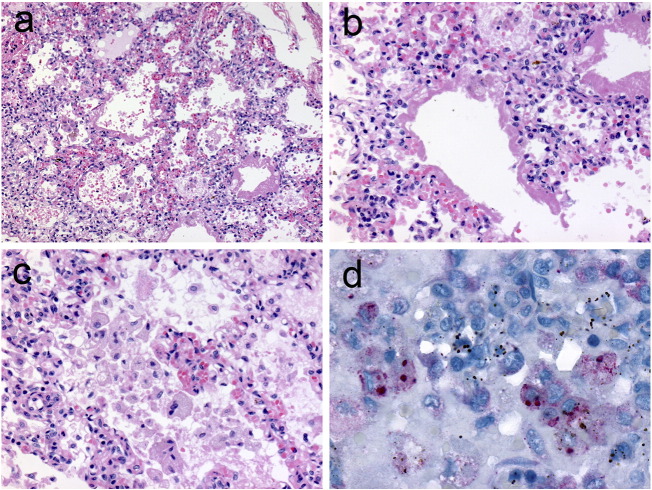
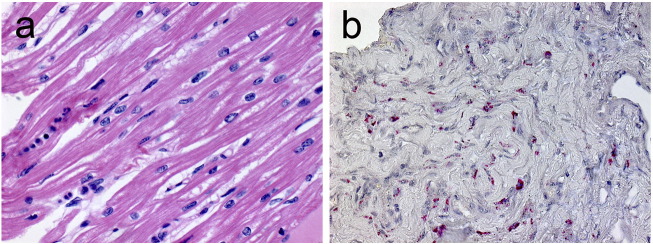
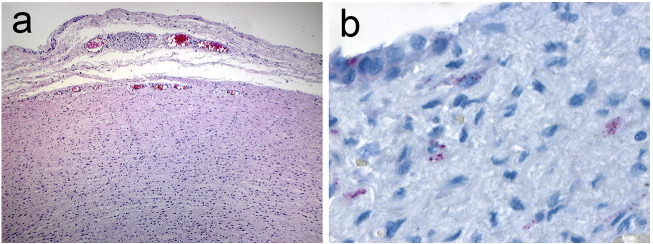
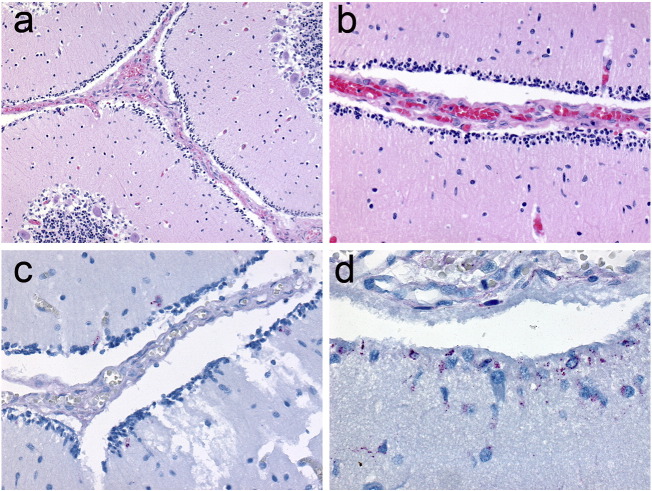
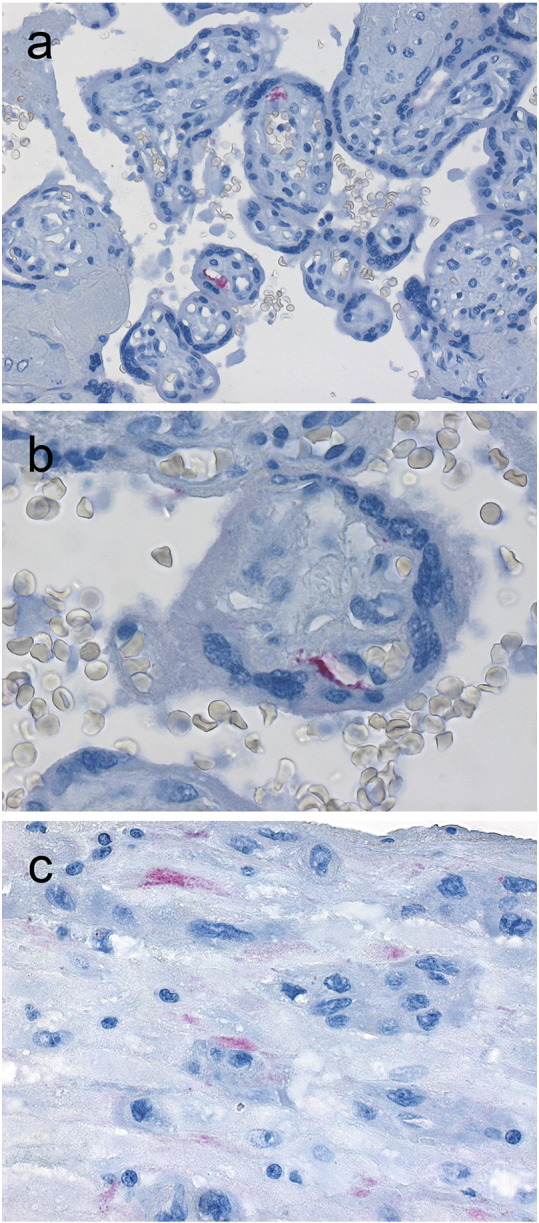
Results: RV antigen was found in interstitial fibroblasts in the heart, adventitial fibroblasts of large blood vessels, alveolar macrophages, progenitor cells of the outer granular layer of the brain, and in capillary endothelium and basal plate in the placenta. The antibody specificity was verified by IHC staining of multiple tissue sections from other infectious disease cases. RV infection of each cell type is consistent with abnormalities which have been identified in patients with CRS, in the heart, large blood vessels, and brain. Antigen distribution was consistent with inflammatory response to vascular injury and systemic spread of RV.
Conclusions: The identification of RV positive cell types in CRS is important to better understand the pathology and pathogenesis of CRS.
Keywords: Autopsy; CRS pathology; Congenital rubella syndrome (CRS); Fatal cases; Immunohistochemistry.
Figures
Comment in
-
Localization of Viral Antigens Improves Understanding of Congenital Rubella Syndrome Pathophysiology.EBioMedicine. 2015 Dec 17;3:8-9. doi: 10.1016/j.ebiom.2015.12.015. eCollection 2016 Jan. EBioMedicine. 2015. PMID: 26870811 Free PMC article. No abstract available.
References
-
- Alford C.A., Neva F.A., Weller T.H. Virologic and serologic studies on human products of conception after maternal rubella. N. Engl. J. Med. 1964;271:1275–1281. - PubMed
-
- Andrus J.K., de Quadros C.A., Solorzano C.C., Periago M.R., Henderson D.A. Measles and rubella eradication in the Americas. Vaccine. 2011;29(Suppl. 4):D91–D96. - PubMed
-
- Boner A., Wilmott R.W., Dinwiddie R. Desquamative interstitial pneumonia and antigen–antibody complexes in two infants with congenital rubella. Pediatrics. 1983;72(6):835–839. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
