

Plasma Lactate Dehydrogenase Levels Predict Mortality in Acute Aortic Syndromes: A Diagnostic Accuracy and Observational Outcome Study
- PMID: 26871831
- PMCID: PMC4753927
- DOI: 10.1097/MD.0000000000002776
Plasma Lactate Dehydrogenase Levels Predict Mortality in Acute Aortic Syndromes: A Diagnostic Accuracy and Observational Outcome Study
Abstract
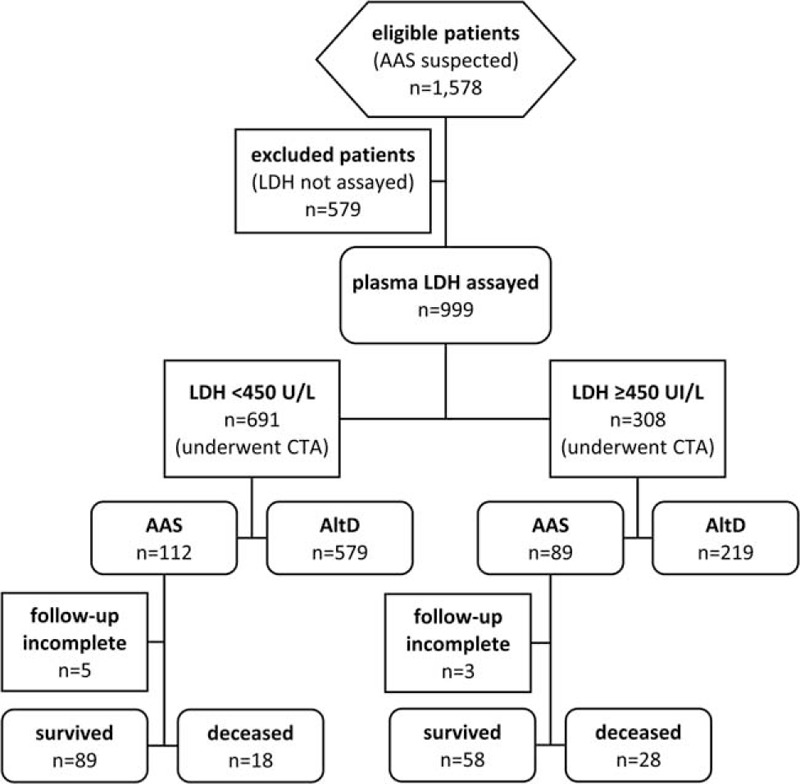
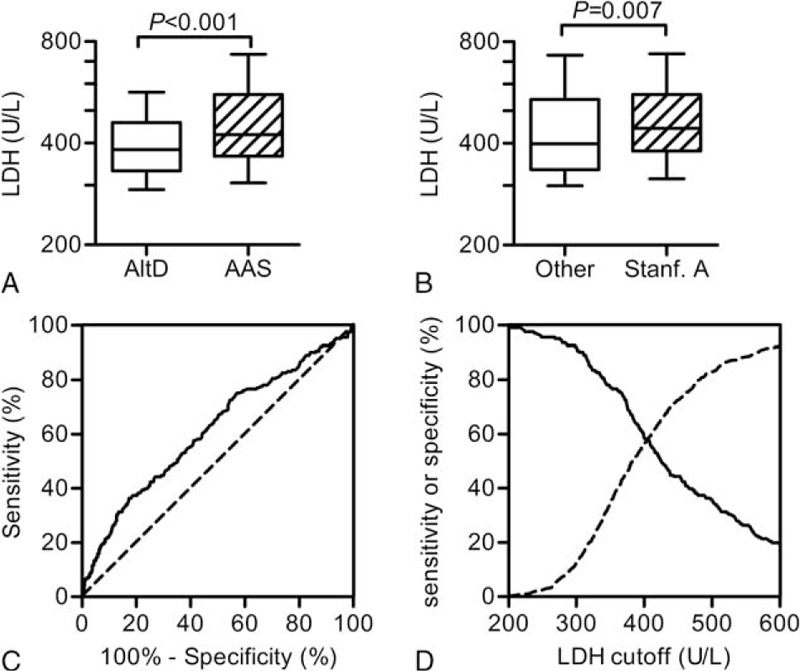
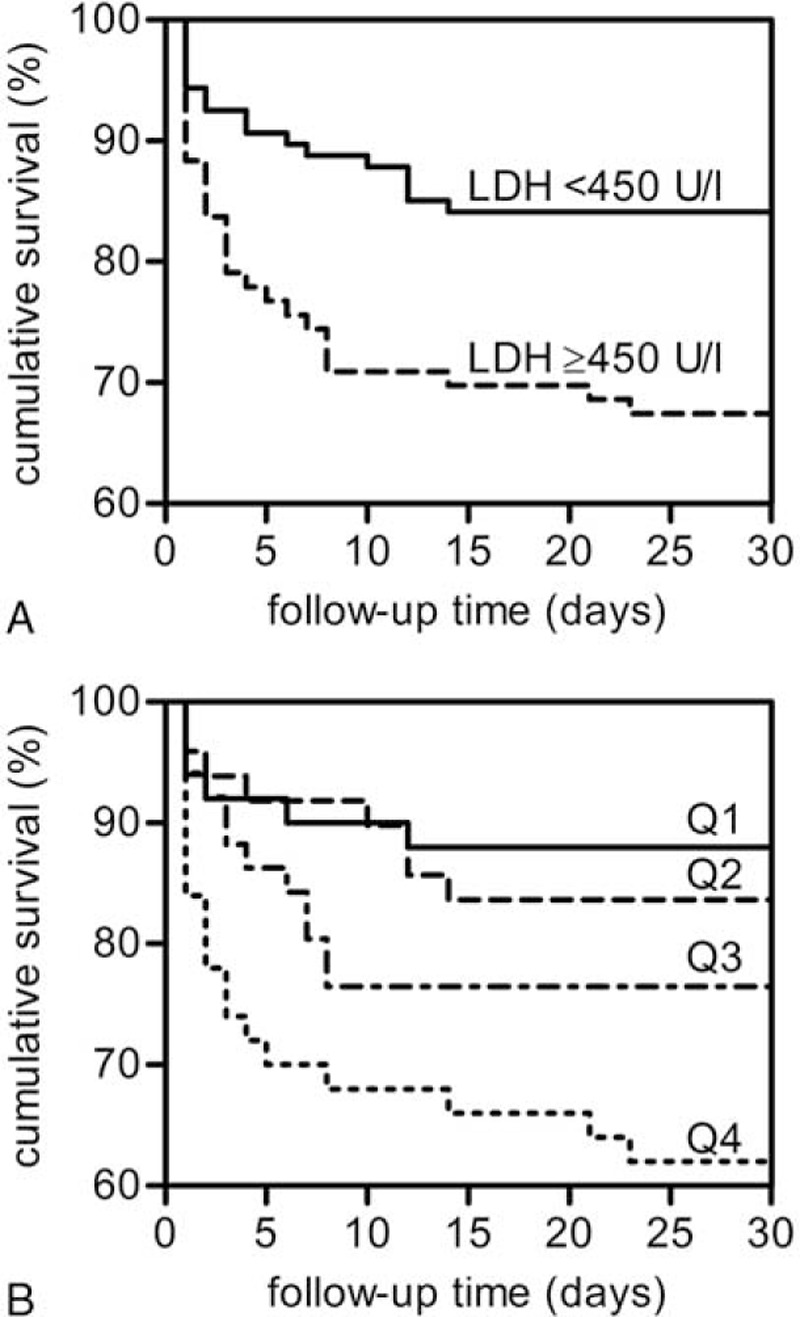
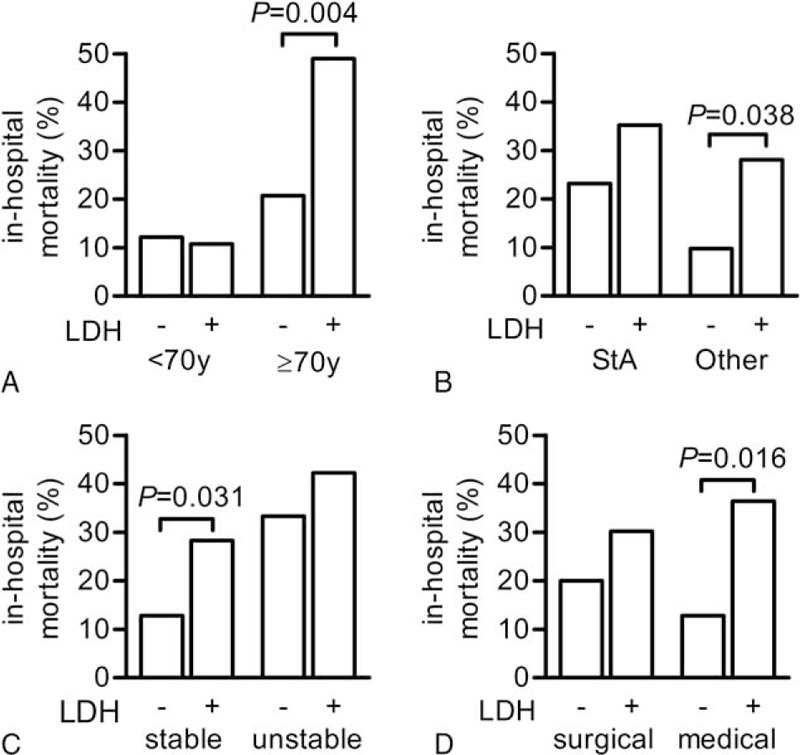
In acute aortic syndromes (AAS), organ malperfusion represents a key event impacting both on diagnosis and outcome. Increased levels of plasma lactate dehydrogenase (LDH), a biomarker of malperfusion, have been reported in AAS, but the performance of LDH for the diagnosis of AAS and the relation of LDH with outcome in AAS have not been evaluated so far.This was a bi-centric prospective diagnostic accuracy study and a cohort outcome study. From 2008 to 2014, patients from 2 Emergency Departments suspected of having AAS underwent LDH assay at presentation. A final diagnosis was obtained by aortic imaging. Patients diagnosed with AAS were followed-up for in-hospital mortality.One thousand five hundred seventy-eight consecutive patients were clinically eligible, and 999 patients were included in the study. The final diagnosis was AAS in 201 (20.1%) patients. Median LDH was 424 U/L (interquartile range [IQR] 367-557) in patients with AAS and 383 U/L (IQR 331-460) in patients with alternative diagnoses (P < 0.001). Using a cutoff of 450 U/L, the sensitivity of LDH for AAS was 44% (95% confidence interval [CI] 37-51) and the specificity was 73% (95% CI 69-76). Overall in-hospital mortality for AAS was 23.8%. Mortality was 32.6% in patients with LDH ≥ 450 U/L and 16.8% in patients with LDH < 450 U/L (P = 0.006). Following stratification according to LDH quartiles, in-hospital mortality was 12% in the first (lowest) quartile, 18.4% in the second quartile, 23.5% in the third quartile, and 38% in the fourth (highest) quartile (P = 0.01). LDH ≥ 450 U/L was further identified as an independent predictor of death in AAS both in univariate and in stepwise logistic regression analyses (odds ratio 2.28, 95% CI 1.11-4.66; P = 0.025), in addition to well-established risk markers such as advanced age and hypotension. Subgroup analysis showed excess mortality in association with LDH ≥ 450 U/L in elderly, hemodynamically stable and in nonsurgically treated patients.Plasma LDH constitutes a biomarker of poor outcome in patients with AAS. LDH is a rapid and universally available assay that could be used to improve risk stratification and to individualize treatment in patient groups where options are controversial.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures
References
-
- Hiratzka LF, Bakris GL, Beckman JA, et al. 2010 ACCF/AHA/AATS/ACR/ASA/SCA/SCAI/SIR/STS/SVM guidelines for the diagnosis and management of patients with thoracic aortic disease: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines, American Association for Thoracic Surgery, American College of Radiology, American Stroke Association, Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and Interventions, Society of Interventional Radiology, Society of Thoracic Surgeons, and Society for Vascular Medicine. Circulation 2010; 121:e266–e369. - PubMed
-
- Erbel R, Aboyans V, Boileau C, et al. 2014 ESC guidelines on the diagnosis and treatment of aortic diseases: document covering acute and chronic aortic diseases of the thoracic and abdominal aorta of the adult. The Task Force for the Diagnosis and Treatment of Aortic Diseases of the European Society of Cardiology (ESC). Eur Heart J 2014; 35:2873–2926. - PubMed
-
- Hansen MS, Nogareda GJ, Hutchison SJ. Frequency of and inappropriate treatment of misdiagnosis of acute aortic dissection. Am J Cardiol 2007; 99:852–856. - PubMed
-
- Stewart A, Chikwe J. Thinking beyond the tube graft: using malperfusion as a guide to define treatment of type A dissection. J Am Coll Cardiol 2015; 65:2636–2637. - PubMed
-
- Czerny M, Schoenhoff F, Etz C, et al. The impact of pre-operative malperfusion on outcome in acute type A aortic dissection: results from the GERAADA registry. J Am Coll Cardiol 2015; 65:2628–2635. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
