

Colonic response to laxative ingestion as assessed by MRI differs in constipated irritable bowel syndrome compared to functional constipation
- PMID: 26871949
- PMCID: PMC4949702
- DOI: 10.1111/nmo.12784
Colonic response to laxative ingestion as assessed by MRI differs in constipated irritable bowel syndrome compared to functional constipation
Abstract
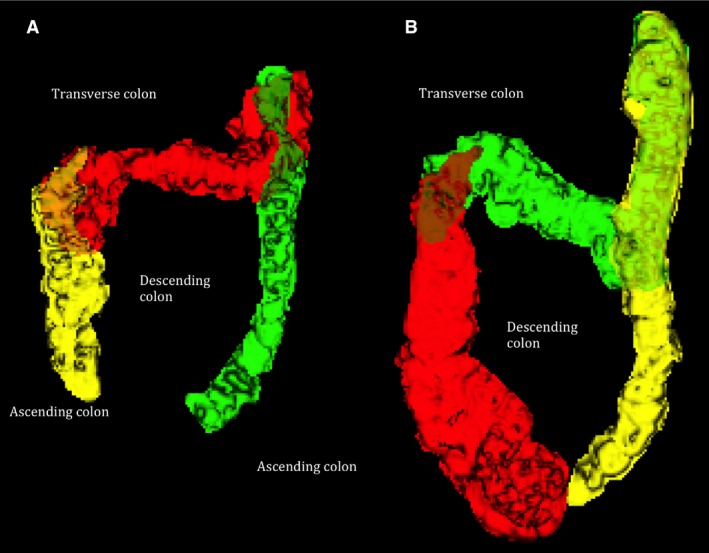
Background: Functional constipation (FC) and irritable bowel syndrome with constipation (IBS-C) share many symptoms but underlying mechanisms may be different. We have developed a magnetic resonance imaging (MRI) technique to measure intestinal volumes, transit, and motility in response to a laxative, Moviprep(®) . We aim to use these biomarkers to study the pathophysiology in IBS-C and FC.
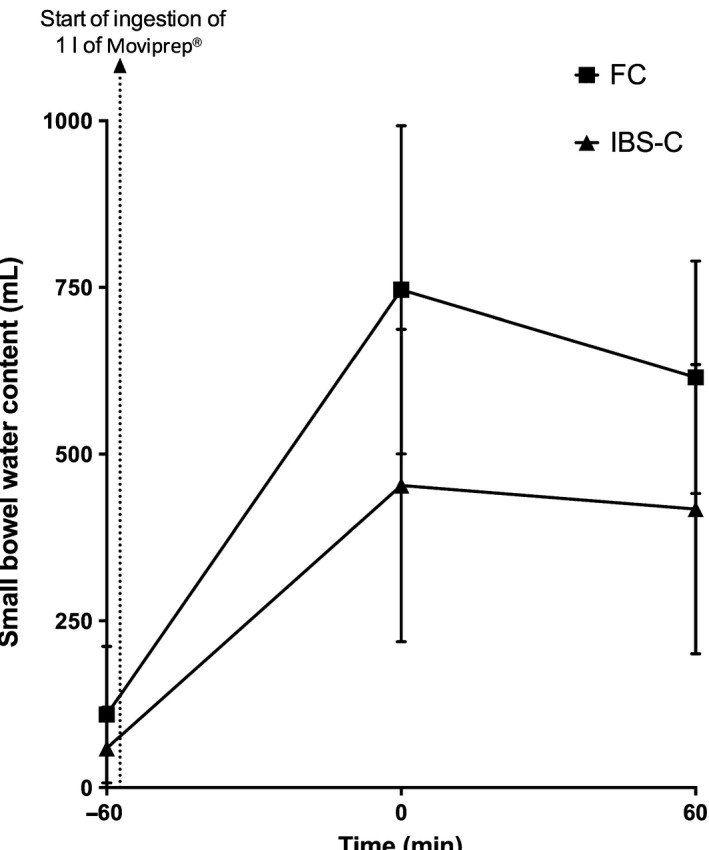
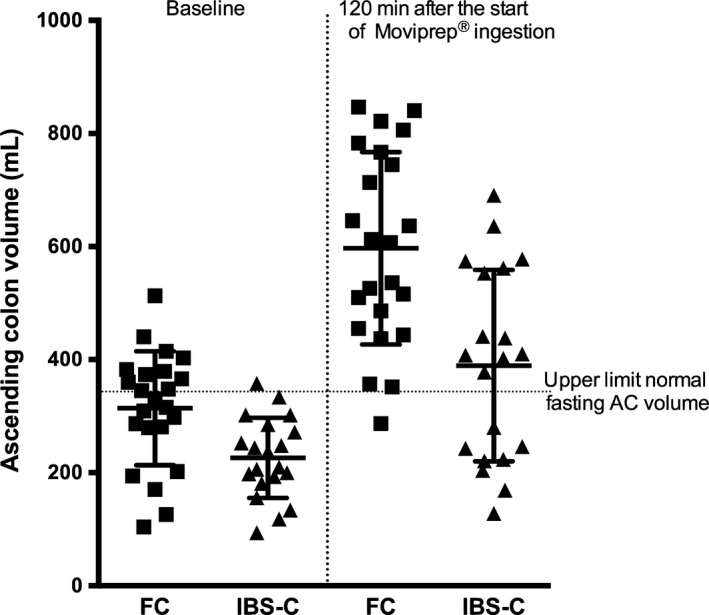
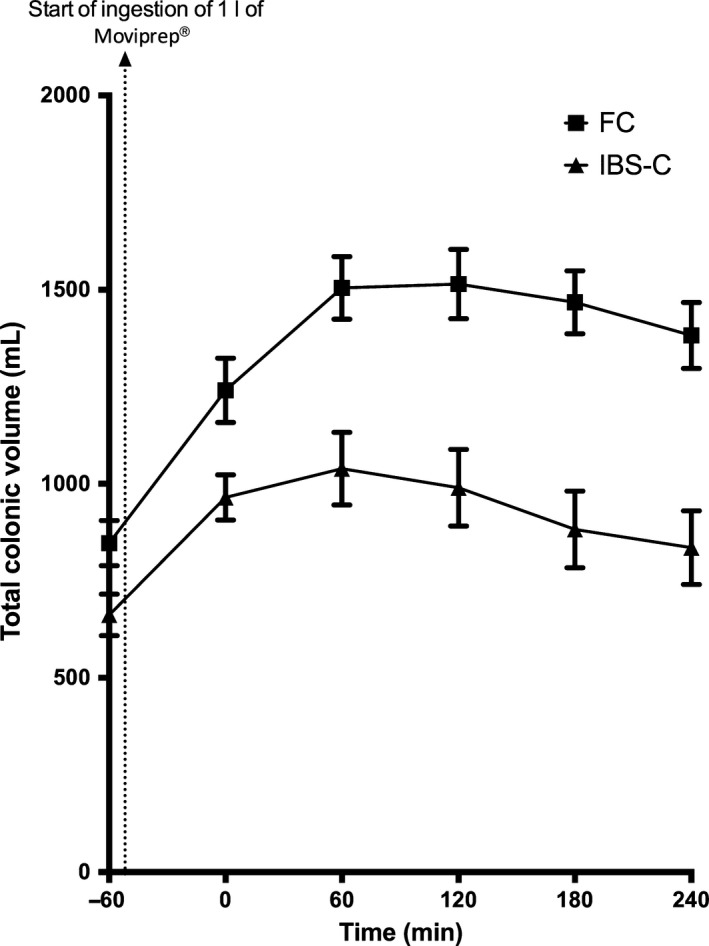
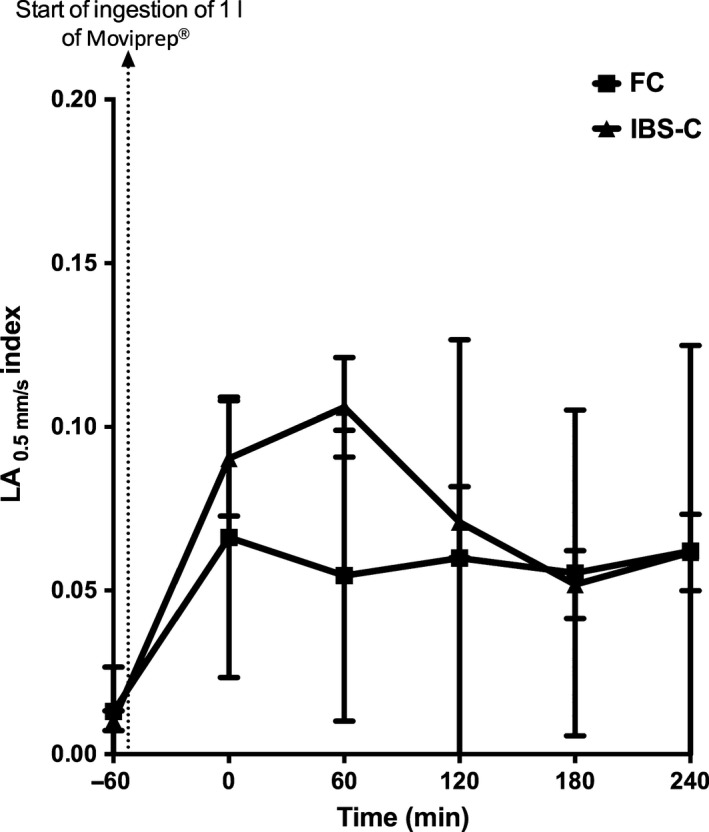
Methods: Twenty-four FC and 24 IBS-C were studied. Transit was assessed using the weighted average position score (WAPS) of five MRI marker pills, taken 24 h before MRI scanning. Following baseline scan, participants ingested 1 L of Moviprep(®) followed by hourly scans. Magnetic resonance imaging parameters and bowel symptoms were scored from 0 to 4 h.
Key results: Weighted average position score for FC was 3.6 (2.5-4.2), significantly greater than IBS-C at 2.0 (1.5-3.2), p = 0.01, indicating slower transit for FC. Functional constipation showed greater fasting small bowel water content, 83 (63-142) mL vs 39 (15-70) mL in IBS-C, p < 0.01 and greater ascending colon volume (AC), 314 (101) mL vs 226 (71) mL in IBS-C, p < 0.01. FC motility index was lower at 0.055 (0.044) compared to IBS-C, 0.107 (0.070), p < 0.01. Time to first bowel movement following ingestion of Moviprep(®) was greater for FC, being 295 (116-526) min, compared to IBS-C at 84 (49-111) min, p < 0.01, and correlated with AC volume 2 h after Moviprep(®) , r = 0.44, p < 0.01. Using a cut-off >230 min distinguishes FC from IBS-C with low sensitivity of 55% but high specificity of 95%.
Conclusion & inferences: Our objective MRI biomarkers allow a distinction between FC and IBS-C.
Keywords: colon; functional constipation; irritable bowel syndrome with constipation; laxative; motility.
© 2016 The Authors. Neurogastroenterology & Motility published by John Wiley & Sons Ltd.
Figures
References
-
- Higgins PD, Johanson JF. Epidemiology of constipation in North America: a systematic review. Am J Gastroenterol 2004; 99: 750–9. - PubMed
-
- Johanson JF, Kralstein J. Chronic constipation: a survey of the patient perspective. Aliment Pharmacol Ther 2007; 25: 599–608. - PubMed
-
- Longstreth GF, Thompson WG, Chey WD, Houghton LA, Mearin F, Spiller RC. Functional bowel disorders. Gastroenterology 2006; 130: 1480–91. - PubMed
-
- Rao SS, Sadeghi P, Beaty J, Kavlock R. Ambulatory 24‐hour colonic manometry in slow‐transit constipation. Am J Gastroenterol 2004; 99: 2405–16. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
