

Low Vitamin-D Levels Combined with PKP3-SIGIRR-TMEM16J Host Variants Is Associated with Tuberculosis and Death in HIV-Infected and -Exposed Infants
- PMID: 26872154
- PMCID: PMC4752266
- DOI: 10.1371/journal.pone.0148649
Low Vitamin-D Levels Combined with PKP3-SIGIRR-TMEM16J Host Variants Is Associated with Tuberculosis and Death in HIV-Infected and -Exposed Infants
Abstract
Background: This study examined the associations of 25-hydroxyvitamin D and specific host genetic variants that affect vitamin D levels or its effects on immune function, with the risk of TB or mortality in children.
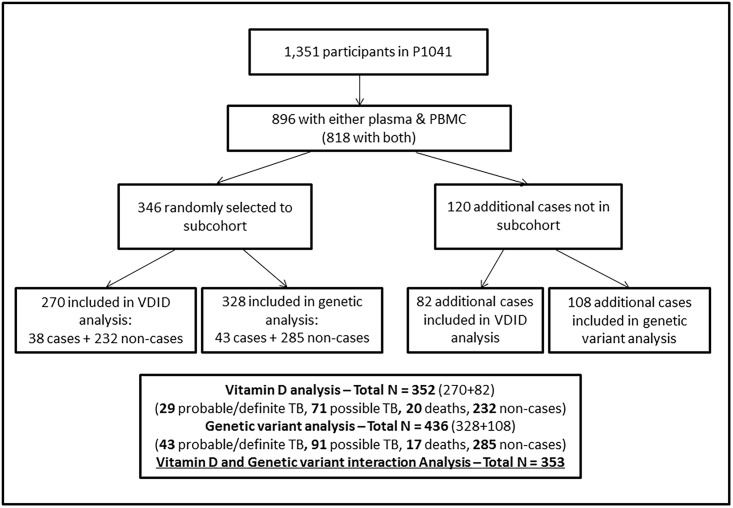
Methods: A case-cohort sample of 466 South African infants enrolled in P1041 trial (NCT00080119) underwent 25-hydroxyvitamin D testing by chemiluminescent immunoassay. Single nucleotide polymorphisms (SNPs) that alter the effect of vitamin D [e.g. vitamin D receptor (VDR)], vitamin D levels [e.g. vitamin D binding protein (VDBP)], or toll like receptor (TLR) expression (SIGIRR including adjacent genes PKP3 and TMEM16J) were identified by real-time PCR. Outcomes were time to TB, and to the composite of TB or death by 192 weeks of follow-up. Effect modification between vitamin D status and SNPs for outcomes was assessed.
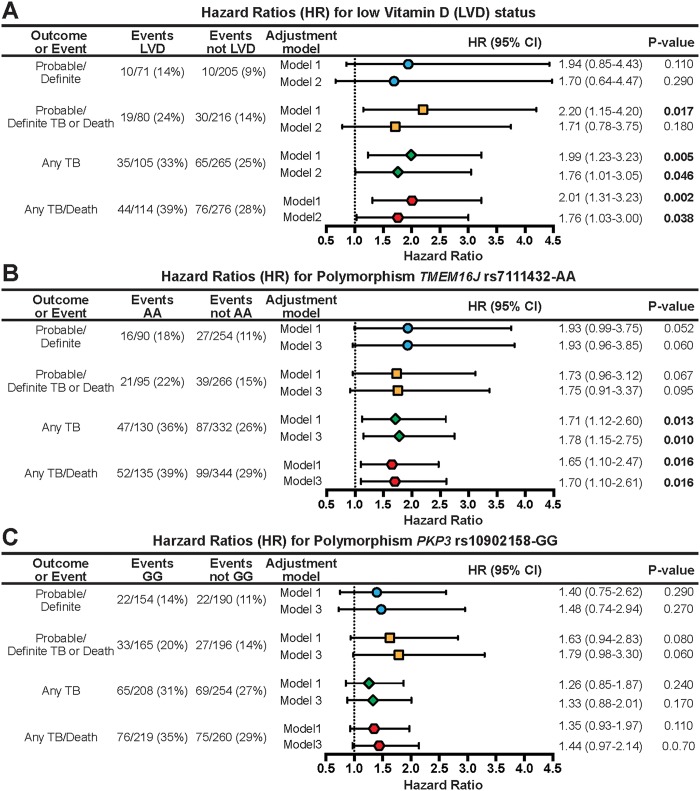
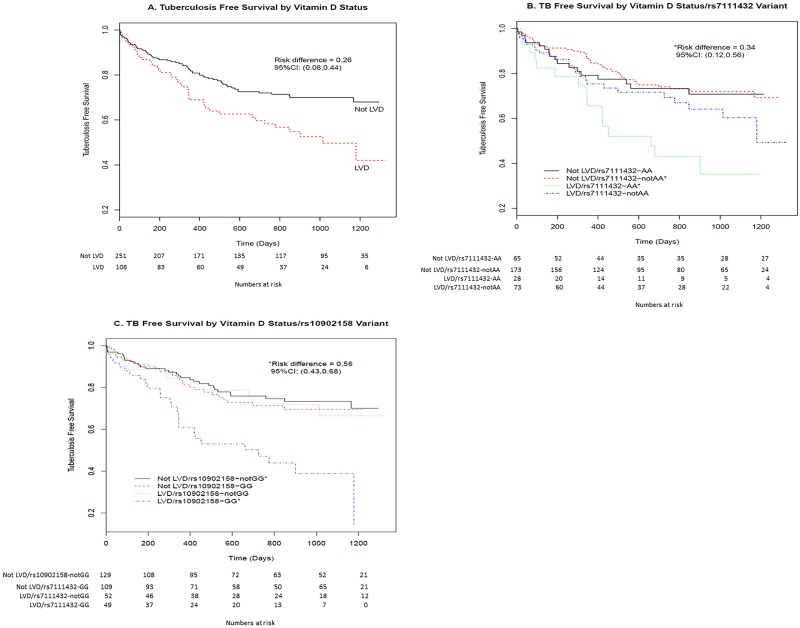
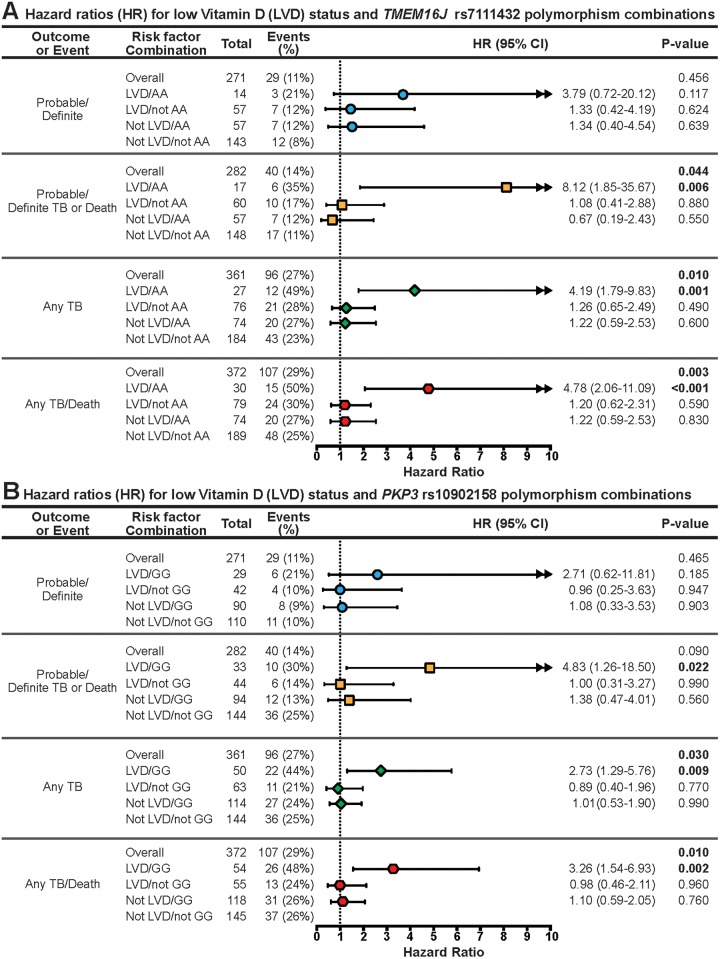
Findings: Median age at 25-hydroxyvitamin D determination was 8 months; 11% were breastfed, 51% were HIV-infected and 26% had low 25-hydroxyvitamin D (<32ng/mL). By 192 weeks, 138 incident TB cases (43 definite/probable, and 95 possible) and 26 deaths occurred. Adjusting for HIV status and potential confounders, low 25-hydroxyvitamin D was associated with any TB (adjusted hazard ratio [aHR] 1.76, 95% CI 1.01-3.05; p = 0.046) and any TB or death (aHR 1.76, 95% CI 1.03-3.00; p = 0.038). Children with low 25-hydroxyvitamin D and TMEM 16J rs7111432-AA or PKP3 rs10902158-GG were at increased risk for probable/definite TB or death (aHR 8.12 and 4.83, p<0.05) and any TB or death (aHR 4.78 and 3.26, p<0.005) respectively; SNPs in VDBP, VDR, and vitamin D precursor or hydroxylation genes were not. There was significant interaction between low 25-hydroxyvitamin D and, TMEM 16J rs7111432-AA (p = 0.04) and PKP3 rs10902158-GG (p = 0.02) SNPs.
Conclusions: Two novel SNPs, thought to be associated with innate immunity, in combination with low vitamin D levels were identified as increasing a young child's risk of developing TB disease or death. Identifying high-risk children and providing targeted interventions such as vitamin D supplementation may be beneficial.
Trial registration: ClinicalTrials.gov NCT00080119.
Conflict of interest statement
Figures
Similar articles
-
Common polymorphisms in the PKP3-SIGIRR-TMEM16J gene region are associated with susceptibility to tuberculosis.J Infect Dis. 2012 Feb 15;205(4):586-94. doi: 10.1093/infdis/jir785. Epub 2012 Jan 5. J Infect Dis. 2012. PMID: 22223854 Free PMC article.
-
Vitamin D deficiency associates with susceptibility to tuberculosis in Pakistan, but polymorphisms in VDR, DBP and CYP2R1 do not.BMC Pulm Med. 2016 May 10;16(1):73. doi: 10.1186/s12890-016-0240-2. BMC Pulm Med. 2016. PMID: 27160686 Free PMC article.
-
Higher serum 25-hydroxyvitamin D concentrations are associated with active pulmonary tuberculosis in hospitalised HIV infected patients in a low income tropical setting: a cross sectional study.BMC Pulm Med. 2018 May 8;18(1):67. doi: 10.1186/s12890-018-0640-6. BMC Pulm Med. 2018. PMID: 29739378 Free PMC article. Clinical Trial.
-
Vitamin D and tuberculosis.Nutr Rev. 2009 May;67(5):289-93. doi: 10.1111/j.1753-4887.2009.00195.x. Nutr Rev. 2009. PMID: 19386033 Review.
-
Vitamin D in Human Immunodeficiency Virus Infection: Influence on Immunity and Disease.Front Immunol. 2018 Mar 12;9:458. doi: 10.3389/fimmu.2018.00458. eCollection 2018. Front Immunol. 2018. PMID: 29593721 Free PMC article. Review.
Cited by
-
The association between vitamin D status and tuberculosis in children: A meta-analysis.Medicine (Baltimore). 2018 Aug;97(35):e12179. doi: 10.1097/MD.0000000000012179. Medicine (Baltimore). 2018. PMID: 30170465 Free PMC article. Review.
-
Vitamin D status and risk of incident tuberculosis disease: A nested case-control study, systematic review, and individual-participant data meta-analysis.PLoS Med. 2019 Sep 11;16(9):e1002907. doi: 10.1371/journal.pmed.1002907. eCollection 2019 Sep. PLoS Med. 2019. PMID: 31509529 Free PMC article.
-
Malnutrition: Modulator of Immune Responses in Tuberculosis.Front Immunol. 2017 Oct 18;8:1316. doi: 10.3389/fimmu.2017.01316. eCollection 2017. Front Immunol. 2017. PMID: 29093710 Free PMC article. Review.
-
Tuberculosis susceptibility and protection in children.Lancet Infect Dis. 2019 Mar;19(3):e96-e108. doi: 10.1016/S1473-3099(18)30157-9. Epub 2018 Oct 12. Lancet Infect Dis. 2019. PMID: 30322790 Free PMC article. Review.
-
The role of vitamin D and the VDR gene polymorphism in sepsis risk and mortality: a systematic review and meta-analysis.Osong Public Health Res Perspect. 2025 Jun;16(3):211-222. doi: 10.24171/j.phrp.2025.0006. Epub 2025 Apr 29. Osong Public Health Res Perspect. 2025. PMID: 40300767 Free PMC article.
References
-
- Hesseling AC, Cotton MF, Jennings T, Whitelaw A, Johnson LF, Eley B, et al. High incidence of tuberculosis among HIV-infected infants: evidence from a South African population-based study highlights the need for improved tuberculosis control strategies. Clinical infectious diseases: an official publication of the Infectious Diseases Society of America. 2009;48(1):108–14. 10.1086/595012 . - DOI - PubMed
-
- WHO. Global Tuberculosis Report Geneva, Switzerland: World Health Organization; 2013.
-
- Graham SM, Ahmed T, Amanullah F, Browning R, Cardenas V, Casenghi M, et al. Evaluation of tuberculosis diagnostics in children: 1. Proposed clinical case definitions for classification of intrathoracic tuberculosis disease. Consensus from an expert panel. J Infect Dis. 2012;205 Suppl 2:S199–208. 10.1093/infdis/jis008 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
- UM1AI106716/AI/NIAID NIH HHS/United States
- HHSN267200800001G/DK/NIDDK NIH HHS/United States
- UM1 AI068632/AI/NIAID NIH HHS/United States
- M01 RR016587/RR/NCRR NIH HHS/United States
- 5R01NS077874/NS/NINDS NIH HHS/United States
- UM1AI068632/AI/NIAID NIH HHS/United States
- HHSN267200800001C/HD/NICHD NIH HHS/United States
- UM1 AI069453/AI/NIAID NIH HHS/United States
- R01 NS077874/NS/NINDS NIH HHS/United States
- UM1 AI068616/AI/NIAID NIH HHS/United States
- UM1AI069465/AI/NIAID NIH HHS/United States
- UM1AI068616/AI/NIAID NIH HHS/United States
- UM1 AI069465/AI/NIAID NIH HHS/United States
- UM1 AI106716/AI/NIAID NIH HHS/United States
- UM1 AI069536/AI/NIAID NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
